Japanese People Had Fewer Heart Attacks Because of These Two Foods
- Normal Liver Cells Found to Promote Cancer Metastasis to the Liver
- Nearly 80% Complete Remission: Breakthrough in ADC Anti-Tumor Treatment
- Vaccination Against Common Diseases May Prevent Dementia!
- New Alzheimer’s Disease (AD) Diagnosis and Staging Criteria
- Breakthrough in Alzheimer’s Disease: New Nasal Spray Halts Cognitive Decline by Targeting Toxic Protein
- Can the Tap Water at the Paris Olympics be Drunk Directly?
Japanese People Had Fewer Heart Attacks Because of These Two Foods
- Should China be held legally responsible for the US’s $18 trillion COVID losses?
- CT Radiation Exposure Linked to Blood Cancer in Children and Adolescents
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- How long can the patient live after heart stent surgery?
Japanese People Had Fewer Heart Attacks Because of These Two Foods
One of the reasons believed to make Japanese people less prone to atherosclerosis, or hardening of the arteries, is the abundance of good HDL cholesterol.
According to a 2008 study comparing the lipid concentrations in the blood of Japanese and Caucasian Americans, while the levels of bad LDL cholesterol and neutral fats were almost the same, the good HDL cholesterol in Caucasian Americans was 10% lower than that in Japanese people.
Good HDL cholesterol not only removes excess cholesterol but also extracts oxidized LDL cholesterol, transporting it to the liver. It has been reported to have additional effects, such as preventing the oxidation of bad LDL cholesterol and protecting the cells inside the blood vessels.
Both in Japan and abroad, the focus on heart attacks has shifted from having too much bad LDL cholesterol to having too little good HDL cholesterol.
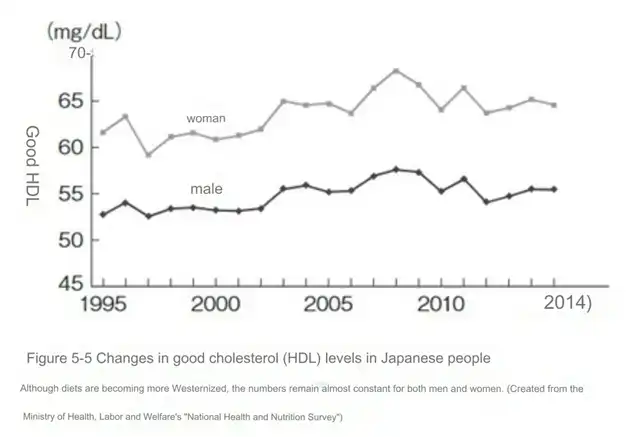
Despite the ongoing Westernization of diets in Japan, there was concern among experts that the reduction in good HDL cholesterol might lead to an increase in atherosclerosis and heart diseases. However, recent findings from the Ministry of Health, Labour and Welfare’s “National Health and Nutrition Survey” reveal that, despite the Westernization of diets, the levels of HDL cholesterol in Japanese people have not decreased.
Figure 5-5 illustrates the values of HDL cholesterol in Japanese men and women, showing relatively constant levels for both genders. Exploring the reasons behind the high levels of HDL in Japanese people could potentially bring significant benefits to people worldwide in preventing atherosclerosis.
Another factor contributing to the low incidence of atherosclerosis in the Japanese population is fish. As mentioned earlier, the bad LDL cholesterol bus carries not only cholesterol but also fatty acids as passengers. Fatty acids, found in all types of fats, are broadly classified into unsaturated fatty acids and saturated fatty acids. The type of fatty acid present in the bad LDL cholesterol bus determines the overall susceptibility to oxidation.
The fatty acids on the bad LDL cholesterol bus are typically unsaturated fatty acids, such as linoleic acid and arachidonic acid. Unsaturated fatty acids are highly susceptible to oxidation, and when they oxidize, the entire bad LDL cholesterol bus becomes oxidized LDL, leading to atherosclerosis.
However, it has been revealed that the bad LDL cholesterol bus in Japanese people contains a higher amount of unsaturated fatty acids, specifically EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid), which actually prevent atherosclerosis. The significance of EPA came to light in the 1970s through research conducted in Greenland, where the indigenous people who consumed a diet rich in seals and fish had lower rates of heart disease. Subsequent studies confirmed a similar trend among the Japanese population.
Both EPA and DHA are unsaturated fatty acids, so they can undergo oxidation. However, EPA and DHA are less prone to oxidation in water, and in fact, they prevent the oxidation of other fatty acids. Although the exact mechanism is not fully understood, as the body is filled with water, the strengths of EPA and DHA are maximized.
EPA and DHA are abundant in fish, especially in blueback fish like mackerel, sardines, saury, and mackerel. EPA, among other functions, suppresses the synthesis of neutral fats and promotes their breakdown, reducing the neutral fats in the body. It also helps prevent the formation of blood clots that can lead to coronary artery blockages. DHA reduces not only neutral fats but also bad LDL cholesterol, without affecting good HDL cholesterol. Since neutral fats make bad LDL cholesterol smaller and more prone to oxidation, reducing neutral fats makes atherosclerosis less likely to occur.
Japanese people, who traditionally consume a lot of fish, are believed to have a transformation in the passengers on the bad LDL cholesterol bus from linoleic acid and arachidonic acid to EPA and DHA, preventing atherosclerosis. In a cohort study of 40,000 Japanese individuals, the group with the highest intake of EPA and DHA had a 40% lower incidence of heart diseases, including heart attacks, compared to the group with the lowest intake.
Although Japanese people are known for their high fish consumption and low incidence of heart diseases globally, increasing the intake of fish could further reduce the risk of heart diseases. The effects of EPA and DHA have been confirmed in Western populations as well, and currently, lipid disorder medications containing concentrated unsaturated fatty acids from fish are used in dozens of countries worldwide, including Europe and the United States.
The Ministry of Health, Labour and Welfare not only suggests that EPA and DHA prevent atherosclerosis but also lower the incidence of other conditions such as diabetes, breast cancer, colorectal cancer, liver cancer, certain types of dementia, and age-related macular degeneration, among others. They recommend a daily intake of 1g of EPA and DHA combined.
The per capita consumption of fish and seafood in Japan remains among the highest globally. According to surveys in 2006 and 2007, Japanese people ingest four times more EPA and DHA than Caucasian Americans. However, due to changes in dietary habits, the consumption of fish continues to decrease. Additionally, the preference for fish with lower EPA and DHA content, such as salmon and tuna, over fatty fish like mackerel and sardines, has caused a steady decline in daily EPA intake since its peak in 1975. To prevent atherosclerosis by eating fish, it is crucial to consider these factors.
However, there is no need to be overly concerned. Even without supplements, consuming 50g of fatty fish per day, equivalent to four pieces of saury nigiri or one slice of grilled mackerel, is sufficient. Both EPA and DHA are abundant in fish skin and the dark meat, so enjoy salt-grilled or simmered fish thoroughly. Obtaining EPA and DHA through daily life by consuming fish has no upper limit.
Another essential food in the Japanese diet contributing to the prevention of heart attacks is soy. While the overall intake of soy in Japan is significantly higher than in other countries, groups with higher soy consumption among the Japanese have shown a two-thirds reduction in the incidence of stroke and about half the incidence of heart attacks compared to groups with lower soy intake, as revealed by a large-scale study conducted among Japanese individuals. Unfortunately, this effect was observed only in women, and there was no such effect in men. This is believed to be due to the isoflavones present in soy, which have functions similar to the female hormone estrogen.
Figure 5-7 displays the daily intake of isoflavones and the international comparison of mortality rates due to heart attacks. This survey, conducted over almost 20 years from 1983, estimated the intake of isoflavones from the amount excreted in urine. Regions with higher isoflavone intake showed a tendency towards lower mortality rates from heart attacks.
The action of isoflavones is much weaker than that of actual female hormones and does not last long. Therefore, it is recommended to consume soy products daily. While this information may prompt consideration of supplements, whether supplements can achieve the same effects has not been conclusively proven.
Soy contains various beneficial components in addition to isoflavones, and their effects may be enhanced when consumed together. For example, lecithin in soy,
Japanese People Had Fewer Heart Attacks Because of These Two Foods
References:
https://news.yahoo.co.jp/articles/e09ddd094bea29b07b51b7b96be88032777b418d
(source:internet, reference only)
Disclaimer of medicaltrend.org
Important Note: The information provided is for informational purposes only and should not be considered as medical advice.



