Targets and prospects for malignant glioma cell therapy
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
- Statins Lower Blood Lipids: How Long is a Course?
- Warning: Smartwatch Blood Sugar Measurement Deemed Dangerous
- Mifepristone: A Safe and Effective Abortion Option Amidst Controversy
- Asbestos Detected in Buildings Damaged in Ukraine: Analyzed by Japanese Company
Targets and prospects for malignant glioma cell therapy
- Red Yeast Rice Scare Grips Japan: Over 114 Hospitalized and 5 Deaths
- Long COVID Brain Fog: Blood-Brain Barrier Damage and Persistent Inflammation
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- How long can the patient live after heart stent surgery?
Targets and prospects for malignant glioma cell therapy
Foreword
Glioma is a devastating disease of the central nervous system, and despite intensive research over the past few decades, the standard of care ( SOC ) for glioblastoma is still limited to resection and chemoradiotherapy.
Immune checkpoint inhibition has shown significant clinical benefit for solid tumors of the peripheral system.
However, none of the phase 3 clinical trials using checkpoint inhibitory molecules in glioma have reached newly diagnosed or recurrent glioblastoma ( GBM ) patients with the primary clinical endpoint.
At present, cell therapy has become an emerging field of clinical cancer research.
With the advent of high-throughput sequencing technologies, tumor antigens and corresponding T cell receptors ( TCRs ) and antibodies are identified, facilitating the development of adoptive T cell therapies including chimeric antigen receptor ( CAR ) T cells.
CAR-T cell therapy has shown excellent therapeutic effect in the treatment of hematological tumors. At present, a large number of CARs have been designed and tested in glioma, which have good therapeutic prospects.
Targets for CAR-T cell therapy in glioma
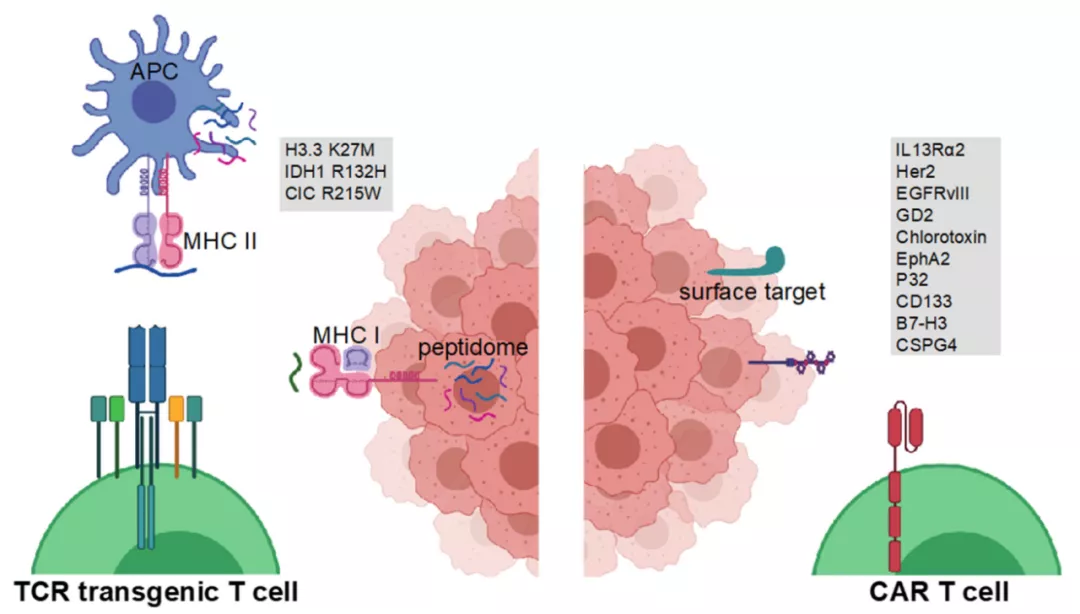
IL13Ra2
IL-13 receptor subunit alpha-2 ( IL13Ra2 ) is the first target in GBM for CAR-T cell therapy.
IL13Ra2 is highly expressed on tumor cells of GBM patients, but at low levels in healthy tissues ( except testis ), making it a suitable target for targeted therapy.
The first CAR targeting IL13Ra2 was developed in 2004 and consisted of an extracellular altered IL13 domain linked to the immunoglobulin transmembrane domain and a CD3 zeta intracellular portion.
Subsequent second-generation CARs included the co-stimulatory 4-1BB domain, which outperformed the first-generation CARs.
Further improvements, such as the addition of activation-induced IL-15 expression to CAR-T cells, resulted in CAR-T cell proliferation, cytokine production, and sustained increases.
The first in vivo clinical trial evaluating IL13Ra2-specific CAR-T was completed in 2015, enrolling three patients with recurrent GBM.
Overall, the treatment was well tolerated in these patients, with only transient brain inflammatory events, suggesting that the T cell product was well tolerated.
Notably, a reduction in tumor IL13Ra2 expression following CAR-T treatment was reported in one patient, indicating a treatment-driven loss of antigen.
Intracerebroventricular IL13Ra2 CAR-T cell therapy is currently being evaluated in Phase 1 clinical trials in ependymoma, GBM and medulloblastoma ( NCT04661384 ), while intratumoral administration is ongoing in relapsed or refractory malignant glioma test ( NCT02208362 ).
HER2
Human epidermal growth factor receptor 2 ( Her2 ) is expressed in approximately 80% of GBM patients.
Her2-specific CAR-T cells demonstrated preclinical efficacy in several tumor models and were shown to efficiently target Her2-positive glioma cells and glioma stem cells, and lead to regression of GBM xenografts.
Recently, it has been reported that Her2-specific CAR-NK cells derived from the human NK cell line NK-92 can specifically lyse GBM-derived cell lines and show in vivo antitumor activity in xenograft and immunocompetent mouse models. This Her2 CAR-NK cell is currently being studied in a Phase 1 clinical trial ( NCT03383978 ).
In addition, in GBM, a Phase 1 dose-escalation study using HER2-specific CAR-T cells derived from virus-specific T cells ( VSTs ) showed good tolerance in 17 patients with no dose-limiting toxic effects. However, HER2-VST CARs did not expand in peripheral blood and had limited clinical efficacy, with a mean OS of 11.1 months.
EGFRvIII
Epidermal growth factor receptor variant III ( EGFRvIII ) is derived from an amplification of wild-type EGFR and is expressed in approximately 30% of GBM patients.
Vaccine or antibody therapy against EGFRvIII has been shown to improve survival and long-term immune memory in various preclinical models, suggesting that EGFRvIII could be an effective target for cell therapy.
The feasibility of targeting CAR-T with EGFRvIII has been extensively studied. In 2017, O’Rourke and colleagues published the first human study using EGFRvIII to target CAR-T.
Ten patients received a single peripheral injection of CAR-T cells.
The results show that CAR-T cells can be efficiently transported to the brain, however, CAR-T cell infiltration leads to an increase in the abundance of Treg cells, inhibiting molecules such as programmed death ligand 1 ( PD-L1 ), transforming growth factor ß ( TGF- ß ) and increased expression of IL10.
Recently, clinical trials of EGFRvIII-specific CAR-T cells targeting intracranial tumors, including GBM , were terminated before completion due to lack of funding, observed toxicity, or lack of objective clinical response ( NCT01454596, NCT02664363, NCT02209376, NCT0328363 1).
GD2
Disialoganglioside ( GD2 ) is frequently overexpressed in neuroblastoma and only limitedly expressed in healthy tissue, which can be classified as a tumor-associated antigen.
CAR-T cell therapy is able to clear tumor progression in xenograft models. Anti-GD2 CAR-T cells also showed great preclinical efficacy in the PDX model of H3.3.K27M.
However, along with the strong antitumor effect, severe neuroinflammation was also observed in immunodeficient mice.
GD2 CAR-T cell therapy is currently being tested in a Phase 1 clinical trial ( NCT04196413 ) in diffuse midline glioma , with three of four patients showing significant improvement in neurological deficit as well as radiographic improvement.
In addition, no on-target non-tumor toxicity was observed. Others include combination with constitutively active IL7 receptor ( NCT04099797 ) and testing in recurrent glioma ( NCT03423992 ).
Chlorotoxin
Chlorotoxin is a venom-derived peptide that specifically binds GBM cells.
Recently, researchers developed a Chlorotoxin-based CAR-T that efficiently targets tumors with heterogeneous expression of GBM-associated antigens such as IL13Rα2, HER2, and EGFR .
Notably, Chlorotoxin-based CAR-T requires the expression of matrix metalloproteinase 2 ( MMP2 ) on tumor cells for efficient binding.
Currently, patients are being recruited for a Phase 1 clinical trial ( NCT04214392 ) evaluating CAR-T cells with the tumor-targeting domain of Chlorotoxin in MMP2-positive relapsed or progressive GBM.
EphA2
Ephrin Type A receptor 2 ( EphA2 ) is a receptor tyrosine kinase that binds to EphrinA family ligands and its downstream signaling is involved in migration, proliferation, differentiation and integrin-mediated adhesion.
It is seen as a glioma-associated antigen with limited expression in healthy tissues, except in certain epithelial cells.
Several preclinical studies used EphA2-directed CAR-T cells to treat GBM xenografts and showed potent antitumor activity against glioma cells.
However, to date, clinical studies evaluating EphA2-targeted CAR-T cells have not been initiated.
P32
P32, also known as C1QBP, has been reported to be expressed in tumor cells and tumor-associated endothelial cells.
Recently, Rousso Noori et al. reported that P32 is specifically expressed on mouse and human glioma cells. In their study, CAR-T cell therapy was able to reduce tumor growth in xenograft and syngeneic mouse models.
Further development of P32 as a CAR-T cell target can be expected.
CD133
CD133 is a five-transmembrane glycoprotein mainly expressed in cancer, hematopoietic and neural stem cells. In hematopoietic stem cell-humanized NOD scid γ ( NSG ) mice, intraventricular injection of CD133-specific CAR-T cells was shown to be effective and did not result in a reduction in the frequency of CD34CD133 double-positive hematopoietic cells.
So far, no phase 1 clinical trials using CD133-specific CAR-T cells have been initiated.
CSPG4
Chondroitin sulfate proteoglycan 4 ( CSPG4 ) is a type I transmembrane protein that is overexpressed in 67% of GBMs.
GBMs with high CSPG4 expression are considered to be more aggressive than those with low CSPG4 expression.
Specific and cell-ratio-dependent killing was observed when CSPG4-specific CAR-T cells were co-cultured with CSPG4-expressing primary GBM cell lines or injected in vivo in human GBM-bearing nude mice.
In these PDX models, no relevant post-treatment antigen loss was observed. So far, there are no clinical trials targeting CSPG4 in gliomas.
B7-H3
B7 homologue 3 ( B7-H3 ) is a type I transmembrane protein that is overexpressed in 76% of GBMs.
Using an established human glioma cell line in nude mice, intratumoral injection of B7-H3-specific CAR-T cells produced durable responses that were independent of the application of costimulatory domains.
Recently, B7-H3 has been successfully applied to B7-H3-CD70 tandem dual-target CAR-T cells. Improved preclinical survival was observed with dual-targeted CAR-T cell therapy compared to single-targeted CD70 or B7-H3.
Currently, patients are being recruited for three clinical trials investigating B7-H3-specific CAR-T in relapsed or refractory GBM or various other central nervous system ( CNS ) tumors.
Overcoming resistance to CAR-T cell therapy
Gliomas represent a highly immunosuppressive microenvironment, therefore, CAR-T cell combination therapy using immunomodulatory agents is imperative.
Agliardi et al. reported that intratumoral application of IL-12 increased the response to EGFRvIII CAR-T cell therapy by enhancing cytotoxicity and remodeling the tumor microenvironment to a more inflammatory state.
Anti-GD2 CAR-T cells have been modified with the IL-15 cytokine domain, and CAR-expressing T cells showed prolonged antitumor activity after repeated antigen exposure, overcoming depletion.
Furthermore, in GBM xenografts, temozolomide enhanced CAR-T cell expansion and persistence and prolonged survival in tumor-bearing mice.
Antigen loss is considered a common tumor escape mechanism when targeting only a single tumor antigen.
Some reports show improved efficacy of CAR-T cell products and reduced resistance to CAR therapy when multiple antigens are targeted.
However, targeting CAR-T cells to multiple targets also increases the risk of off-target effects, and clinical trials targeting multiple antigens have not yet been initiated.
Typically, downregulation of tumor antigens is mediated through epigenetic silencing.
Therefore, it is tempting to use epigenetic drugs to modulate epigenetic silencing of CAR-T cell targets. In some solid tumors, DNA methyltransferase blockade combined with CAR-T cell therapy has shown signs of improved efficacy in preclinical models.
In a medulloblastoma xenograft model, the demethylating agent azacytidine resulted in increased targeted expression and prolonged survival after CAR-T cell therapy.
The Prospect of Glioma CAR-T Cell Therapy
The main obstacles to effective cell therapy of brain tumors remain the adequate infiltration, persistence, and resilience of transgenic T cells, as well as overcoming the hostile brain tumor microenvironment.
Recent studies have shown that IDH mutation status is associated with reduced antigen-presenting capacity, especially in IDH-mutated tumor microenvironments where T cells are severely rejected.
The mesenchymal subtype of glioblastoma is considered to be the more immunologically active subtype of glioblastoma, and the specificity of these glioma entities or glioblastoma subtypes suggests that appropriate adjustment of cell therapy may be required.
Current concepts to overcome major hurdles include the use of alternative routes of application and combination therapy in preclinical and early clinical trials.
There is evidence of associated peripheral antigen presentation in brain tumors.
However, so far, it is unclear whether antigen presentation has an impact on the efficacy of local or systemic application of TCR or CAR-T cells in glioma.
If systemic antigen presentation proves to be relevant, the already designed concept of in vivo CAR-T cell boosting based on synthetic vaccines will become important.
Some trials were even terminated before completion in search of a combination therapy, known as immune checkpoint inhibition.
CAR and TCR-T cell therapy have both unique advantages and disadvantages, and the combination of the two cell therapy concepts should be explored preclinically in the near future.
Meanwhile, inducible cell systems are in preclinical development to reduce targeted non-tumor side effects.
Also important for biomarker assessment, prior biopsy or resected tumor tissue should be representative of current tumor disease at the start of therapy.
Summary
Compared with other glioma immunotherapy approaches such as dendritic cell vaccine, peptide vaccine or TIL therapy, CAR and TCR-T cell therapy have their own unique advantages.
Many targets in glioma have been tested in preclinical and clinical studies of CAR-T cell therapy, and many targets show promising application prospects.
With further development of combination therapy and CAR/TCR-T cell therapy itself, adoptive T cell therapy, like other tumors, will show the potential to cure glioma.
references:
1. Genetically Modified Cellular Therapies for Malignant Gliomas. Int J Mol Sci. 2021Dec; 22(23): 12810.
Targets and prospects for malignant glioma cell therapy
(source:internet, reference only)
Disclaimer of medicaltrend.org
Important Note: The information provided is for informational purposes only and should not be considered as medical advice.



