Excimer laser treatment of arteriosclerosis occlusion of lower extremities
- Why Botulinum Toxin Reigns as One of the Deadliest Poisons?
- FDA Approves Pfizer’s One-Time Gene Therapy for Hemophilia B: $3.5 Million per Dose
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
- Statins Lower Blood Lipids: How Long is a Course?
- Warning: Smartwatch Blood Sugar Measurement Deemed Dangerous
Excimer laser treatment of arteriosclerosis occlusion of lower extremities
Excimer laser treatment of arteriosclerosis occlusion of lower extremities. To evaluate the application and value of excimer laser ablation in the treatment of lower extremity arteriosclerosis occlusion.
Method
A retrospective analysis of the basic information and pathological changes of 30 patients (31 limbs) who underwent excimer laser ablation combined with drug-coated balloon (DCB) treatment in the Zhongshan Hospital of Fudan University from June 2019 to March 2020. Features, surgical efficacy and related complications.
Results:
Among the 30 patients, 21 were males and 9 were females. His age was (76.5±10.5) years old, and the length of the lesion was (11.7±6.4) cm. There were 41 lesions, including 12 cases (29.3%) of in-stent restenosis (ISR), 24 cases (58.5%) of chronic occlusive disease (CTO) for initial treatment, and 5 cases (12.2%) of severe stenosis. 51.6% of patients had a grade 4 calcification classification (PACSS). The technical success rate was 93.5%, 4 cases (12.9%) complicated with distal embolization, and 2 cases (6.5%) with salvage stent implantation. Follow-up (6.6±3.0) months, the ankle-brachial index (ABI) increased from 0.43 (0.32, 0.55) before surgery to 0.91 (0.87, 1.01) immediately after surgery (Z=-5.43, P<0.01) and 3 after surgery 0.82 (0.73, 1.02) per month (Z=-3.99, P<0.01). The 3-month amputation-free survival rate was 96.7%, the first-stage patency rate was 100%, the diseased vessel reintervention rate (TLR) was 0, and the ulcer healing rate was 76.9%.
Cconclusion
Excimer laser ablation and volume reduction are both feasible and effective for ISR and initial treatment of CTO. It provides a new option for DCB lumen preparation and reduction of stent implantation.
With the aging of the population and changes in people’s living habits and other factors, the incidence of lower extremity atherosclerotic occlusion (ASO) has increased significantly. With the continuous advancement of treatment technology, intracavitary minimally invasive treatment has increasingly become its mainstream therapy. Percutaneous angioplasty (PTA) and stent implantation are classic surgical procedures for endovascular treatment [1, 2, 3, 4]. In-stent restenosis (ISR) is the main factor affecting its efficacy, reaching 14% to 50% [1, 2, 5, 6].
“Volume reduction” maximizes the gain of the lumen by removing the contents of the lumen, reducing the implantation of arterial stents below the groin, and improving the patency rate, which has become the mainstream and development hotspot of ASO endovascular treatment. The main volume reduction methods currently used in China include: plaque oriented atherectomy (DA), percutaneous thrombus removal (PMT) and excimer laser ablation (ELA). According to the different contents of the vascular cavity, choose the corresponding method: DA is the first choice for plaque, especially calcified plaque, PMT is the first choice for thrombus, and ELA is the first choice for ISR.
But the indications of the three are crossed: for example, Rotarex in DA and PMT can also be applied to ISR, and ELA can also be applied to plaque. Among the three, ELA has been applied and promoted relatively late in China, and there are few reports on the efficacy of Chinese people. This study retrospectively analyzed the data of lower limb ASO patients treated with ELA volume reduction combined with drug-coated balloon (DCB) in Zhongshan Hospital of Fudan University, and summarized and discussed the characteristics and clinical value of ELA.
Object and method
1. General information:
A retrospective analysis of the data of 30 patients with lower extremity ASO lesions who received ELA combined with DCB treatment in Zhongshan Hospital of Fudan University from June 2019 to March 2020. This study was approved by the Ethics Committee of Zhongshan Hospital Affiliated to Fudan University (Y2019-099), and each patient signed an informed consent form before surgery.
2. Inclusion and exclusion criteria:
Standard constrain:
(1) Age from 18 to 85 years old;
(2) Rutherford Grade 3 and above;
(3) Ankle-brachial index (ABI) of the affected limb <0.8;
(4) Iliac, femoral popliteal and inferior knee artery stenosis and occlusive disease; (5) Lower limb arterial ISR, digital subtraction angiography (DSA) or CT angiography (CTA) confirmed in-stent restenosis>50%.
Exclusion criteria:
(1) Life expectancy <1 year;
(2) Contrast agent allergy;
(3) Severe cardiovascular or hepatorenal dysfunction cannot tolerate surgery;
(4) Blood coagulation dysfunction;
(5) The disease cannot be true cavity by.
3. Operation process:
Routinely use local anesthesia in the groin area, and perform surgery on the opposite side through the common femoral artery. Insert 6/7F sheath. Calcification score (PACSS) [7] was performed under direct vision of DSA, and at the same time, the location, nature, length, and outflow tract conditions of the lesion were confirmed by angiography. The 0.035 Terumo/V-18 guide wire is used with the single-curved/supported catheter to pass the pathologically through the true lumen.
Measure the diameter of the blood vessel of the diseased segment, choose the appropriate 0.9~2.5 mm Turbo-Elite catheter (Spectranetics, USA), generally choose the 0.9~2.0 mm catheter for the inferior knee artery, connect the CVX-300 laser generator (Spectranetics, USA) at the end, and adjust The energy density is 35~70 mJ/mm2, and the working frequency is 35~80 Hz. The end of the laser catheter is connected to a pressure pump, and 15 ml of normal saline is injected at a constant rate to flush the blood vessel with contrast agent.
The laser catheter is calibrated at a speed of 1 mm/s Push from the proximal end of the lesion to the distal end, and at the same time inject normal saline at a constant rate of 1 ml/s. If the guide wire cannot pass through the lesion, the “Step-by-step” (SBS) technique can be used, that is, without the aid of the guide wire, each advancement is a short distance (<5 mm) to ablate the lesion. After each ablation, withdraw the laser catheter, and observe whether the lesion has achieved volume reduction effect by angiography, that is, residual stenosis <30%, infinite flow dissection and distal embolism.
If you are not satisfied, you can repeat the above steps again for ablation until a satisfactory lumen is obtained (Figure 1). After the ablation is completed, an ordinary balloon is used for pre-expansion, and then DCB is used to expand the lesion. If there is a restrictive dissection >40% or residual lumen stenosis >30%, a self-expanding stent is implanted. Review the ABI before discharge. After the operation, aspirin (100 mg/d) and clopidogrel (75 mg/d) were routinely taken for 6 months, and then aspirin (100 mg/d) was taken for a long time.
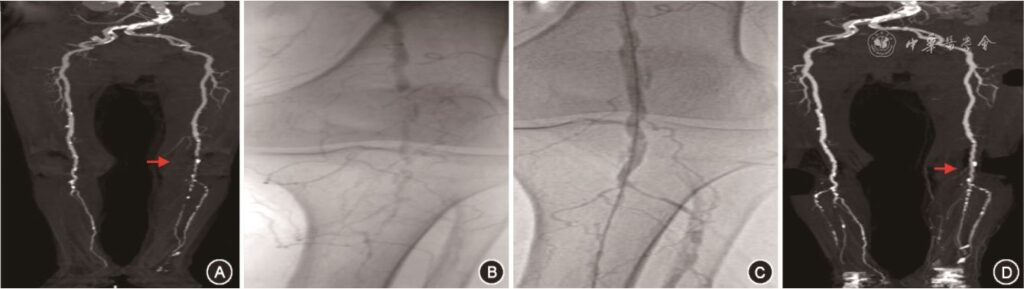
figure 1. Diagnosis and endovascular treatment results of patients with lower extremity arteriosclerosis occlusion A: Preoperative CT angiography (CTA) showed occlusion of P2~3 segments of the left popliteal artery (red arrow); B: Intraoperative angiography confirmed the left popliteal artery P2~3 Segmental occlusion; C: The occluded segment is unobstructed after excimer laser ablation (ELA); D: CTA shows that the ELA treated segment is still unobstructed 4 months after the operation (red arrow)
4. Endpoint events and observation indicators:
the first-stage end-point event is the survival rate without amputation; the second-stage end-point events include salvage stent implantation rate, distal embolization rate, first-stage patency rate, diseased vessel reintervention rate (TLR) and ulcer Healing rate. All patients were followed up for 1, 3 months and every 3 months thereafter. During the follow-up, the patient underwent CTA and ABI examinations. Technical success is defined as: residual stenosis <30% after volume reduction of the diseased vessel, and infinite flow dissection. Definition of postoperative restenosis: CTA or DSA examination showed that the diameter of the diseased artery was ≥50% or ABI decreased >0.2 and symptoms became worse. Definition of the first-stage patency rate: During the follow-up period, no surgical or interventional interventions were used again, and the target blood vessel remained patency.
5. Statistical processing:
All data were collected with Microsoft Excel and statistically analyzed using SPSS 20.0 software. Continuous variables that conform to the normal distribution are represented by x¯±s, the comparison between before and after surgery is by t test, and the categorical variable is represented by the case (%). Continuous variables that do not conform to the normal distribution are represented by M (Q1, Q3), and the comparison between the variables uses the Mann-Whitney U test. Pearson χ² test is used to compare categorical variables. When the expected value of the variable is <5 value> 20% of the cell, Fisher’s exact test is used. The Kaplan-Meier method was used for survival analysis. Both adopt a two-sided test, and the test level is α=0.05.
Results:
1. Basic clinical data:
From June 2019 to March 2020, a total of 30 patients with 31 limbs were included. Among them, 21 cases (70.0%) were male, and their age was (76.5±10.5) years old. Complications included 25 cases of hypertension, 19 cases of diabetes, 9 cases of hyperlipidemia, 6 cases of myocardial infarction, 5 cases of chronic renal insufficiency, and 2 cases of cerebral infarction. According to Rutherford classification, 9 cases were grade 3, 9 cases were grade 4, and 13 cases were grade 5.
There were 19 cases of left side lesions and 12 cases of right side lesions. The length of the lesions was (11.7±6.4) cm. A total of 41 lesions, including the iliac artery in 2 cases (4.9%), the superficial femoral artery in 22 cases (53.7%), the popliteal artery in 12 cases (29.3%), the tibiofibular trunk in 3 cases (7.3%), the posterior tibial and peroneal artery 1 case (2.4%) in each artery. There were 24 cases of chronic occlusion, 12 cases of ISR, and 5 cases of severe stenosis. ELA time is 241 (150,480) s, processing (2.5±0.7) times, and emitting pulses 10 056 (5 843, 20 410) times.
2. Treatment result:
The technical success rate is 93.5% (29/31). Two cases had restrictive dissection, both of which were chronic occlusive disease of the superficial femoral artery (CTO), grade 4 PACSS. Flow-limiting dissection occurred after ELA, and no significant improvement was seen after pre-expansion with a common balloon, so a self-expanding stent was implanted. Distal embolism occurred in 4 (12.9%) cases. The first two cases were long-segment ISR lesions of the superficial femoral artery, and the embolization was in the distal popliteal artery and tibiofibular trunk (Figure 1).
One patient had embolism after the ELA was completed, and there was no obvious distal blood flow restriction, so no treatment was done; the other ISR case had an embolization of the distal tibiofibular shaft during the ELA process, so the SpiderFX umbrella was placed and continued The operation is complete. The third case of embolization was due to severe calcification of the lesion and difficulty in passing the catheter, so that excessive force caused the calcified plaque to fall off and embolize the popliteal artery. Then the frequency of the catheter was reduced, the energy was increased, and the embolic plaque was successfully ablated at a speed of 0.5 mm/s (Figure 2).
The fourth case was subacute thrombosis of ISR from the superficial femoral artery to the first segment of the popliteal artery (P1). The stent distal embolization occurred after ELA. The blood flow was significantly improved after the 4F single-curved catheter was aspirated, but after DCB expansion, the distal The spasm of the end blood vessels appeared, and the papaverine 15 mg bolus was relieved. There was 1 case (3.2%) of vascular perforation. This patient was an ISR lesion of a long superficial femoral artery. At the beginning of ELA, the patient had pain in the groin area, and the angiography showed obvious contrast agent extravasation. Consider the perforation because it is ablated The blood vessels were not flushed with normal saline before, so that the laser catheter was excited in the contrast agent to generate a large amount of energy, which caused the blood vessels to perforate. After stopping the operation, the local pressure improved for 5 minutes.
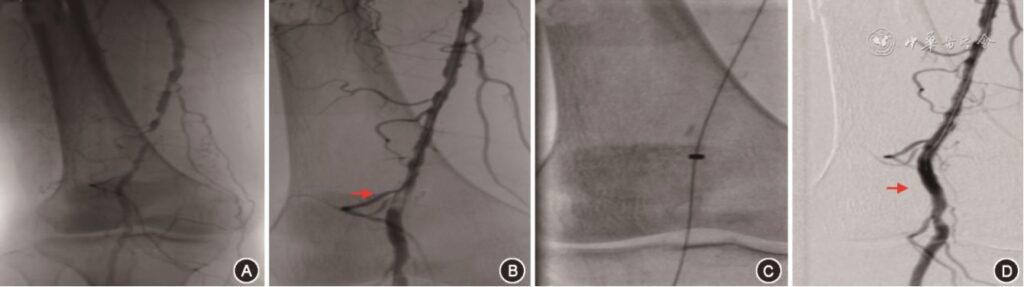
figure 2. Comparison of excimer laser ablation (ELA) before and after treatment in patients with lower extremity arteriosclerosis occlusion A: Intraoperative angiography showed occlusive lesions in the middle and distal part of the right superficial femoral artery; B: The distal end of the lesion was found to be embolized after ELA (red arrow); C: The embolus was treated with ELA again; D: The angiography showed that the embolization site was unobstructed (red arrow)
3. Follow-up:
30 patients were followed up for (6.6±3.0) months, and no follow-up was lost. The first-stage patency rate was 100%, and Kaplan-Meier calculated the 3-month amputation-free survival rate was 96.7%. TLR is 0. ABI increased from 0.43 (0.32, 0.55) before surgery to 0.91 (0.87, 1.01) immediately after surgery (Z=-5.43, P<0.01), and it was 0.82 (0.73, 1.02) at 3 months after surgery (Z=-3.99) , P<0.01). One patient (3.3%) died of pneumonia 9 months after the operation. The area of the ulcer on the treated side limb was significantly reduced before death, and the resting pain was relieved. Thirteen patients (41.9%) had foot ulcers. At present, 10 patients (76.9%) have healed completely, and 3 patients (23.1%) had significantly reduced ulcer area and relieved pain.
Discussion:
The main reasons why volume reduction has become the intracavitary treatment of lower extremity ASO are as follows: (1) It can remove the proliferated intima, thrombus and other substances in the blood vessel to achieve the purpose of obtaining the lumen; (2) It can reduce the flow restriction. The occurrence of sexual dissection; (3) It can make DCB drugs better contact the arterial intima, inhibit its proliferation, and improve the patency rate.
The existing methods for volume reduction in the lower limb ASO cavity mainly include the following: DA, PMT and ELA. DA is a good choice for volume reduction of calcified lesions. Combined with DCB can significantly improve the patency rate of blood vessels [8], but its application is limited by the following factors: (1) The length of the collection bin and the routine need to combine the use of distal embolization protection devices in the lesion There is a 6-10 cm normal blood vessel between the bifurcation of the popliteal artery or the bifurcation of the tibiofibular trunk. Otherwise, the blade may not be able to cut and reduce the volume of the entire lesion due to the blocking of the protective umbrella; (2) due to the volume of the collection chamber Limited, it takes longer to deal with long lesions; (3) For ISR lesions, there is a risk of cutting the stent; (4) The direction needs to be adjusted according to the location of the lesion; (5) The iliac artery is a contraindication for DA. The operation of PMT is relatively convenient, and the combined acute/subacute thrombus can be removed simultaneously. The limitations are: (1) It is not suitable for chronic nonthrombotic lesions of non-stent-covered segments, especially calcification; (2) For vein graft ISR, the risk of injury is relatively high when applied; (3) It is not suitable for popliteal arteries. Beyond the fork.
ELA is the only device approved by the U.S. Food and Drug Administration (FDA) for the treatment of femoral popliteal artery ISR [9]. (1) ELA can not only effectively deal with ISR, but also be compatible with the new lesions at both ends, and there is no need to use a remote umbrella. (2) The scope of ELA work is not limited, covering iliac artery-ankle artery disease. A total of 41 lesions were treated in this study, of which 12 (29.3%) cases of popliteal artery (CTO: 11; severe stenosis: 1), of which 10 cases involved P2~P3 segments. After ELA, satisfactory lumen was obtained and technical success was achieved. (3) No need to adjust the direction. (4) For CTO lesions where the guide wire is difficult to pass through the real cavity, ELA has its unique advantages, that is, the “SBS” technology: the guide wire and the ELA catheter are on the same track and heads together. Then follow up the guide wire alternately, pass the lesion, and establish a channel for the conventional PTA/stent. “SBS” technology is relatively difficult to enter the subendometrium, providing a new option for passing CTO lesions [10].
In this study, a total of 7 (17.1%) patients had complications, including 4 cases of distal embolization, 2 cases of restrictive dissection, and 1 case of vascular perforation. Distal Embolic Event Protection Using Excimer Laser Ablation in Peripheral Vascular Interventions (DEEP EMBOI) studies have shown that compared with PTA/stent, the use of ELA does not increase the probability of distal vascular embolization, so there is no need for routine use of protective umbrellas [11].
In order to reduce the occurrence of distal embolism, the speed of catheter pushing should be less than 1 mm/s; in addition, the catheter should advance at a uniform speed. In case of severe calcification plaques, the frequency and energy can be appropriately increased, and the laser catheter will stop on the plaque and continue to ablate until the catheter can smoothly pass through the calcified lesion. Secondly, for long-segment severe calcification (PACSS level 2 or above) and ISR lesions, if there is only one distal outflow tract, a protective umbrella should be considered to prevent distal embolism.
For acute thrombosis, reduce the frequency and increase the energy to increase the ablation area, or perform intracatheter thrombolysis first, and then use ELA for volume reduction after the thrombotic load is reduced. The occurrence of restrictive dissection is mainly due to calcified plaques [12]. During operation, you can choose a laser catheter with a larger diameter within the allowable range of the blood vessel diameter, such as 2.3 mm or 2.5 mm, to increase the ablation area of the laser probe and improve work efficiency.
In the case of a perforation patient in this study, a sufficient amount of saline was not injected to flush the vascular cavity before the excitation, which caused the laser catheter to be excited in the blood vessel with the residual contrast agent, and the greater energy caused the blood vessel damage. Before and during ELA work, it is necessary to continuously inject physiological saline. On the one hand, in order to empty the contrast agent to avoid damaging the vascular endothelium, at the same time emptying the blood makes the energy more concentrated, and also has the effect of cooling down.
In short, ELA is feasible and effective for ISR and CTO for initial treatment, and provides a new option for DCB lumen preparation and reduction of stent implantation. The shortcomings of this study are the small number of cases and the short follow-up time. However, considering that the application of this technology in some countries has been developed for a short time, it is an emerging technology and can be used as a preliminary research result for clinical reference.
(source:internet, reference only)
Disclaimer of medicaltrend.org



