Current status and challenges of immunotherapy for colorectal cancer
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
- Statins Lower Blood Lipids: How Long is a Course?
- Warning: Smartwatch Blood Sugar Measurement Deemed Dangerous
- Mifepristone: A Safe and Effective Abortion Option Amidst Controversy
- Asbestos Detected in Buildings Damaged in Ukraine: Analyzed by Japanese Company
Current status and challenges of immunotherapy for colorectal cancer
- Red Yeast Rice Scare Grips Japan: Over 114 Hospitalized and 5 Deaths
- Long COVID Brain Fog: Blood-Brain Barrier Damage and Persistent Inflammation
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- How long can the patient live after heart stent surgery?
Current status and challenges of immunotherapy for colorectal cancer.
Preface
Colorectal cancer ( CRC ) is a common malignant tumor, the incidence rate ( 6.1% ) of all cancers ranks third, and the mortality rate ( 9.4% ) ranks second.
Due to the diversity and heterogeneity of colorectal cancer, in addition to surgical resection, there are few effective treatment strategies in recent years.
As immunotherapy has become a revolutionary treatment method after surgery, coupled with chemotherapy and targeted therapy, the treatment of colorectal cancer has ushered in a new stage.
Immune Checkpoint Inhibitor ( ICI ) therapy has become the main anti-colorectal cancer immunotherapy method currently used.
In addition, immunotherapies other than ICIs, such as chimeric antigen receptor modified T ( CAR-T ) cells or immunotherapy based on oncolytic viruses, have emerged rapidly in recent years.
These have promoted the development of immunotherapy for colorectal cancer.
As a new and powerful anti-tumor treatment, immunotherapy will become an alternative treatment strategy for patients with colorectal cancer.
Colorectal cancer classification system
The MMR/MSI system is the most important indicator of CRC classification and is used to formulate treatment strategies.
Microsatellites are tandem repeats of dozens of nucleotides, with one to six nucleotides as repeating units.
Microsatellite instability ( MSI ) is a frameshift mutation of microsatellites in tumor cells caused by the insertion or deletion of repeat units.
The DNA Mismatch Repair ( MMR ) system combats these errors by identifying and repairing DNA damage, and correcting insertions, deletions, or mismatched bases caused by the wrong cycle in the DNA replication process.
MMR is divided into defective mismatch repair function ( dMMR ) and complete mismatch repair function ( pMMR ). dMMR is manifested as a lack of MMR protein.
When the MMR system is dysfunctional or mutated, these genetic errors will not be corrected, so that they are permanently integrated into the tumor DNA, which is called highly unstable ( MSI-H ).
On the contrary, MMR protein is expressed normally in pMMR, which is mainly divided into low degree of instability ( MSI-L ) and stable ( MSS ).
Colorectal cancer dMMR/MSI-H subtype accounts for about 15% of all cases and 5% of mCRC cases.
Due to the high mutation rate of dMMR/MSI-H, the tumor has high immunogenicity, which enables it to activate the anti-tumor effect of the immune system.
Patients with dMMR/MSI-H are more responsive to ICI-based immunotherapy.
Therefore, finding new and more effective immunotherapy strategies to treat different CRC subtypes has become the mainstream.
Treatment strategies for colorectal cancer based on ICI
As an important marker of MMR protein deficiency, MSI stability has become a major indicator for guiding treatment strategies for patients with colorectal cancer.
In recent years, with in-depth research on immune markers, a large number of studies have shown that high TMB can predict the efficacy of ICIs in the treatment of colorectal cancer.
The MMR/MSI classification system also helps to guide the decision-making of immunotherapy strategies for CRC patients.
The treatment strategy of dMMR/MSI-H colorectal cancer
Since most dMMR/MSI-H CRC subtypes have high TMB, ICIs and immunotherapy have excellent therapeutic effects on patients with high TMB.
Therefore, ICI immunotherapy strategy has become the main clinical treatment method for patients with dMMR/MSI-H subtype, including PD-1 inhibitor ( pembrolizumab or nivolumab ) monotherapy, PD-1 inhibitor and CTLA4 inhibitor combination therapy ( nivolumab +ipilimumab ), PD-L1 inhibitor and anti-VEGF antibody combination therapy ( atezolizumab+bevacizumab ).
A clinical study ( NCT02060188 ) recruited 74 patients with MSI-H subtype and treated with nivolumab.
After treatment, about 68.9% of patients had disease control for more than 12 weeks; in addition, 8 patients ( 34.8% ) experienced an immune response lasting more than 12 months, indicating that nivolumab provides long-term response and disease for dMMR/MSI-H mCRC patients control.
More interestingly, in patients with MSI-H subtypes, the combined strategy of ICIs seems to have a greater anti-tumor effect.
In 2018, a study of the combination of nivolumab and ipilimumab in the treatment of MSI-H tumors was conducted.
In 119 patients, the combination therapy achieved 80% effective tumor control at 12 weeks and maintained more than 94% of the immune response.
All these data indicate that the combined strategy of PD-1 inhibitors and CTLA4 inhibitors leads to higher immune response rates and longer overall survival ( OS ) and progression-free survival ( PFS ), prompting the US Food and Drug Administration ( FDA ) approved nivolumab combined with ipilimumab for the treatment of patients with dMMR/MSI-H subtype.
The treatment strategy of pMMR/MSS colorectal cancer
Recently, a randomized trial using PD-L1 and CTLA4 inhibitors durvalumab and tremelimumab, respectively, was used for supportive pMMR/MSS colorectal cancer treatment.
180 patients with colorectal cancer were divided into D+T group ( durvalumab+tremelimumab ) and BSC group ( best supportive treatment ).
Although the objective response rate ( ORR ) of the two groups was similar to PFS, the OS of the D+T group improved. This brings new hope for the immunotherapy of pMMR/MSS mCRC.
However, the clinical benefit is limited to a small percentage of patients with CRC subtypes, accounting for about 4% of all CRC patients. For the pMMR/MSSCRC subtype, ICI treatment cannot achieve the best effect.
When MSI is present, tumor cells release many tumor-associated antigens ( TAA ) usually located in the tumor membrane , which are then absorbed and presented by antigen-presenting cells ( APC ) located in the tumor immune microenvironment , enhancing the anti-tumor ability of T cells.
However, for the pMMR/MSS subtype of colorectal cancer, the DNA structure is too stable to release TAAs, which prevents the immune system from activating or induces activated immune cells to fail to recognize tumor cells.
Therefore, some studies have shown that PD-1 inhibitors have poor efficacy in patients with pMMR/MSS CRC subtypes, and there is an urgent need for new treatment strategies to enhance tumor immunity in patients with pMMR/MSS colorectal cancer.
So far, many studies have shown that chemotherapy, molecular targeted therapy and radiotherapy can cause immunogenic cell death ( ICD ) of cancer cells .
After ICD, tumor cells are exposed to a large amount of TAA, releasing damage-related molecular patterns and pro-inflammatory cytokines, effectively promoting immune cell infiltration and activating APC.
These may provide new immunotherapy strategies for pMMR/MSS colorectal cancer patients with low immune response.
The treatment strategy of pMMR/MSI-L colorectal cancer
For patients with pMMR/MSI-L CRC subtype, the microsatellite stability of cancer cells is between the MSI-H and MSS subtypes.
Therefore, this subtype has almost no specific tumor characteristics. So far, the commonly used immunotherapy strategies for MSI-L subtypes are divided into three categories: CTLA4 inhibitors ( ipilimumab ), PD-1 inhibitors ( pembrolizumab or nivolumab ) and PD-L1 inhibitors ( atezolizumab or durvalumab ) and their combinations.
Therefore, the FDA has approved the combination of pembrolizumab and nivolumab and the combination of nivolumab and ipilimumab for the treatment of CRC.
ICIs are not absolutely effective for MSI-L subtypes. In a 2015 study, it was observed that pembrolizumab treatment did not produce good immune-mediated anti-tumor effects on patients with pMMR/MSI-L tumors.
In addition, in another study, 142 pMMR/MSI-L patients had a limited response to immunotherapy, and only one of 20 patients showed an immune-mediated anti-tumor response to the combination of PD-1 and CTLA4 antibodies.
In recent years, with the discovery of new ICI combination therapy strategies, substantial progress has been made in improving the effectiveness of combined immunotherapy for patients with such tumors.
In a study published in 2015, the combined application of PD-L1 inhibitors and MEK inhibitors showed significant effects on patients with pMMR/MSI-L colorectal cancer. The RAS-MAPK pathway is a transmembrane transduction of growth signals by multiple membrane receptors, and its activation is related to the reduction of tumor infiltration by T cells and directly promotes tumor cell proliferation.
Treatment strategies classified according to the degree of immune cell infiltration
Due to the extensive chromosomal changes and dMMRs in colorectal cancer, there is genetic heterogeneity among different colorectal cancer cells.
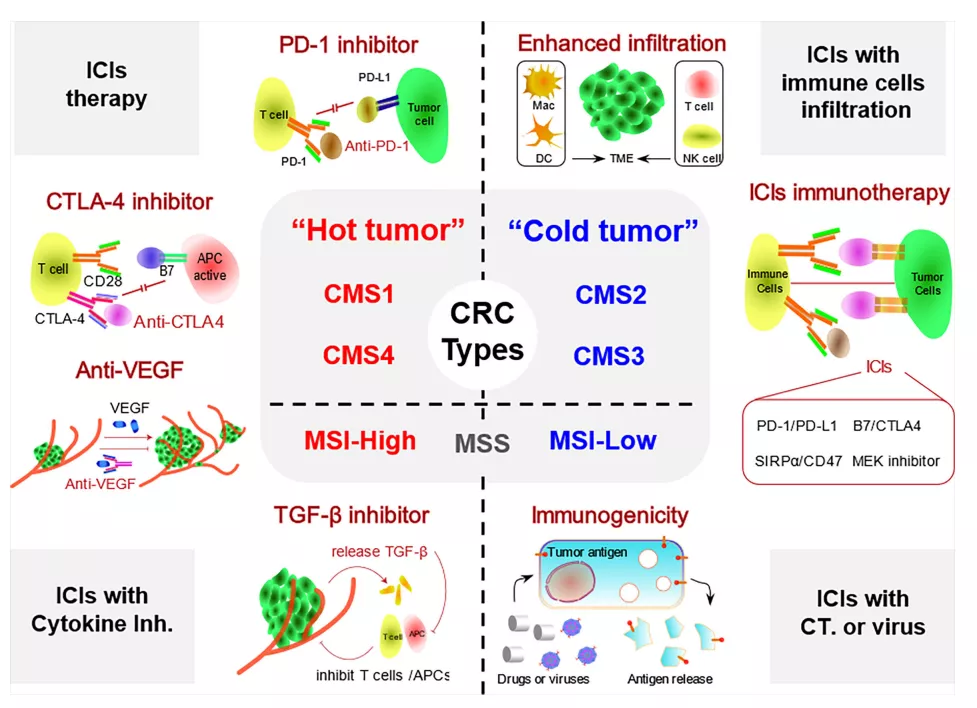
Based on the pathological and molecular biological data of 3000 patients with colorectal cancer, Guinney divided the patients with colorectal cancer into four subtypes: CMS1, microsatellite unstable immunotype ( 14% ), which is characterized by high MSI-H mutations and at the same time Shows BRAF mutations and strong immune cell infiltration; CMS2 is the most common type ( 37% ), which is characterized by WNT and MYC pathway activation and chromosomal instability; CMS3, metabotropic ( 13% ), mainly with KRAS mutations and mixed MSI Status and abnormal metabolic pathways are characteristics; CMS4 is a mesenchymal subtype ( 3% ), which is characterized by activation of the transforming factor TGF-β, enhanced angiogenesis, interstitial infiltration and inflammatory infiltration.
Among the four subtypes, the CMS1 and CMS4 subtypes are characterized by more extensive lymphocyte infiltration and higher distribution of inflammatory cytokines around the tumor, while the CMS2 and CMS3 subtypes have almost no lymphocyte or inflammatory cell infiltration.
Therefore, according to the presence of lymphocyte infiltration and the inflammatory environment around the tumor, the four colorectal cancer subtypes based on the CMS system are artificially divided into two types, hot colorectal cancer and cold colorectal cancer.
Treatment strategies for hot colorectal cancer
TME of febrile colorectal cancer contains many lymphocytes and inflammatory infiltrates, mainly including CMS1 and CMS4 subtypes. CMS1 type is the main potential beneficiary of colorectal cancer immunotherapy.
A 2016 study showed that when a large number of aggressive T cells, especially cytotoxic CD8+ T cells, accumulate in TME, the patient’s PFS and OS will be prolonged.
They detected a large number of infiltrating T cells and B cells in CMS1 subtype tumors, which provided a strong guarantee for the treatment strategy of ICIs.
CMS4 is the second largest subtype, accounting for approximately 23% of the total number of CRC cases.
Mainly manifested as activation of transforming factor TGF-β, enhanced angiogenesis, interstitial infiltration and inflammatory infiltration. However, unlike CMS1, CMS4 has an unfavorable inflammatory immune phenotype, resulting in a poor immune microenvironment, and active T cells cannot kill tumor cells.
Therefore, treatment strategies for ICIs are rarely studied in the CMS4 subtype. Selective TGF-β inhibitors combined with ICIs may help immunotherapy for CMS4 patients.
In addition, CMS4 promotes angiogenesis in the microenvironment and increases the expression of VEGF-related factors ( such as FGF ).
The method of eliminating VEGF or reducing its expression and release has become another research direction. Currently, many clinical studies are investigating the efficacy of VEGF inhibitors combined with ICI on colorectal cancer.
Treatment strategies for cold colorectal cancer
CMS2 and CMS3 subtypes are the main representative types of cold colorectal cancer. CMS2 subtype is the most common subtype, accounting for about 37% of all CRC cases.
The main feature of CMS2 and CMS3 subtypes is the lack of tumor immunogenicity of TME.
Studies have shown that ICIs alone are not effective, which is related to the immunosuppressive properties of cold colorectal cancer.
At present, a variety of immunotherapy strategies have been developed, such as oncolytic viruses, cytokine therapy, CAR-T therapy and passive immunotherapy against TAAs.
These strategies are helpful for immune activation anti-tumor therapy of cold tumors.
Chemoimmunotherapy strategy
ICIs have always been the most mature and effective immunotherapy methods for colorectal cancer.
However, it appears to be limited to CRC subtypes with low immunogenicity or low immune cell infiltration.
Therefore, immunotherapy with ICIs alone is not effective for certain subtypes of CRC, and chemoimmunotherapy has become an important strategy for the treatment of colorectal cancer.
In order to further improve the survival rate of colorectal cancer patients treated with FOLFOX or FOLFIRI strategy, a new GOLFIG strategy has been developed.
This strategy combines low-dose recombinant IL-2 and GM-CSF on the basis of FOLFOX and the chemotherapy drug gemcitabine.
In the GOLFLG strategy, a variety of chemotherapeutic drugs can successfully destroy tumor cells in large quantities, and rIL-2 and GM-CSF will promote the activation of APC, and then activate CTL to accurately destroy the remaining tumor cells.
Correale and others first explored the effect of the FOLFIG trial.
They found that the remission rate and disease control rate of mCRC patients were higher than that of the FOLFOX strategy, indicating significant immune response and anti-tumor activity.
Oncolytic virus and CAR-T cell therapy
In recent decades, oncolytic virus therapy has attracted more and more attention, and related research has also made great progress.
The oncolytic vaccinia virus ( VV ) treatment strategy has been proven to transform colorectal cancer-type cold tumors into hot tumors by promoting the infiltration of immune cells, thereby generating effective anti-tumor immunity.
However, the therapeutic potential of oncolytic viruses is also affected by the immunosuppression of tumors on immune cells, such as immune checkpoints.
According to the research published by Wei, the strategy of combining VV with anti-TIGIT monoclonal antibody has played a better role in reducing tumor burden and prolonging survival compared with oncolytic VV therapy alone.
In short, oncolytic virus combined with ICIs may be a new direction for the treatment of colorectal cancer.

For CMS2 and CMS3 CRC subtypes, low-level immune cell infiltration is the main factor leading to poor immune response.
The emergence of CAR-T cell therapy has become the main and precise treatment strategy to solve this problem. In 2017, Zhang et al. conducted a phase I clinical trial of CAR-T treatment for colorectal cancer with high CEA expression ( NCT02349724 ).
In this trial, 10 patients with colorectal cancer received 5 increasing doses of CAR-T cell therapy, and no serious adverse events related to CAR-T therapy were observed during the follow-up period.
Seven of the 10 patients progressed during the previous treatment, but their condition was stable after CAR-T treatment. Imaging analysis showed that the tumors shrank in two patients after treatment.
In 2019, Ying et al. loaded the truncated CD19 ( CD19T ) gene into oncolytic viruses to increase the expression of CD19 antigen on the surface of tumor cell membranes. At the same time, they combined CAR-T immunotherapy with the chimeric CD19 gene to enhance the specific targeting effect of CAR-T.
The combination of oncolytic virus and truncated CD19 ( OV-CD19T ) specifically replicates and expresses CD19T antigen in different solid tumor cells.
The combination therapy of OV-CD19T and CD19-CAR-T is safe and effective in vitro and in vivo The method of treating solid tumors suggests that it has a long-lasting tumor killing effect.
Cancer Immunization Vaccine
Therapeutic cancer vaccines containing TAAs or tumor-specific antigens ( TSAs ) can directly stimulate the immune system and activate CD4+ and CD8+ T cells to kill tumors.
Many cancer vaccines have been developed, including cell vaccines, nucleic acid vaccines, protein peptide vaccines and genetic engineering vaccines.
Thymidylate synthase multi-epitope peptide ( TSPP ) is an anti-cancer multi-epitope peptide vaccine that can promote the cross-presentation of tumor antigens through APC and trigger a highly specific immune response with multi-antigen specificity.
TSPP has shown good anti-tumor activity in preclinical studies of colorectal cancer.
In addition, immunotherapy response is usually related to TMB, and dMMR/MSI-H patients have higher genetic mutation characteristics.
Therefore, vaccines against specific gene mutation-related antigens have been shown to be effective for this type. In 2017, Maletzki and others constructed a dMMR mouse model induced by MLH1 gene knockout.
After the mice were injected with dMMR cancer vaccine, the OS time was prolonged and the tumor mutation load was reduced, indicating that specific vaccines are feasible for the treatment of dMMR subtypes. choose.
Immune adjuvant
Immune adjuvant is a kind of non-specific immune proliferation agent, is an adjuvant that effectively activates antigen immune response or changes the type of immune response, and is of great significance for improving the immunotherapy effect of colorectal cancer.
At present, immune adjuvants are mainly divided into biological adjuvants and non-biological adjuvants. Biological adjuvants have good immunosensitization effects.
In a phase I clinical trial, the use of Mn 2+ combined with anti-PD-1 antibodies safely improved the anti-tumor efficacy of advanced mCRC treatment.
From 2018 to 2019, Lv et al. initiated a phase I clinical trial on the effect of Mn 2+ on advanced mCRC. In this study, by intranasal or inhalation, the clinical ORR after treatment with MnCl2 solution was 45.5%, and the tumor control rate was 90.9%.
More importantly, 5 patients who had previously failed anti-PD-1 antibodies or chemotherapy combined with radiotherapy showed good DCR during the treatment period, indicating that Mn 2+ restored the immunotherapy effect of immunotherapy resistant patients.
As an inorganic adjuvant, Mn 2+ has undoubtedly become the most important immunosensitizer in colorectal cancer immunotherapy. It may activate the immune response of immunotherapy-resistant colorectal cancer patients and provide a new and more effective treatment Strategy.
Challenges of immunotherapy for colorectal cancer
As an effective treatment strategy following surgery, radiotherapy, chemotherapy and targeted therapy, immunotherapy strategies have shown strong anti-tumor efficacy and strong therapeutic potential in the treatment of colorectal cancer.
However, as an emerging treatment method , there are still many challenges in terms of safety and effectiveness.
For ICI treatment strategies, although some CRC subtypes show good therapeutic effects, for other CRC subtypes, such as pMMR/MSS and dMMR/MSI-L, the effect is not ideal. It is necessary to develop more new ICI portfolio strategies by exploring its specific mechanisms.
On the other hand, due to the heterogeneity of solid tumors and the external microenvironment, the effect of solid tumor immunotherapy is not as good as expected.
The low clinical targeted response rate and the risk of autoimmune diseases are still the main limiting factors.
Overactive immune system during treatment may cause serious adverse reactions in patients with colorectal cancer.
In recent years, more and more ICIs combination therapies have been developed, which solves some of the limitations of ICIs only used for the treatment of colorectal cancer.
However, although more immunotherapy strategies for colorectal cancer are being developed, there is still no detailed classification for the characteristics of the immune environment of colorectal cancer.
A more meaningful method is to formulate classification based on different immune response characteristics of colorectal cancer.
Summary
At present, improving the immunogenicity of tumors while increasing the targeting of the immune system and improving the invasiveness of immune cells have become an important treatment strategy for enhancing the immunotherapy of colorectal cancer. Including chemotherapy, targeted therapy, oncolytic virus, CAR-T therapy, the combined application of tumor vaccines and checkpoint inhibitors has become an important direction in the future.
In short, as the most promising anti-tumor treatment at present, immunotherapy has great potential as a treatment strategy for colorectal cancer, which may bring new hope to colorectal cancer patients.
references:
1. Progress in the Application of ImmuneCheckpoint Inhibitor-Based Immunotherapy for Targeting Different Types of Colorectal Cancer. Front Oncol. 2021; 11: 764618.
Current status and challenges of immunotherapy for colorectal cancer.
(source:internet, reference only)
Disclaimer of medicaltrend.org
Important Note: The information provided is for informational purposes only and should not be considered as medical advice.



