Why does MRI often underestimate the size of prostate tumors?
- A Single US$2.15-Million Injection to Block 90% of Cancer Cell Formation
- WIV: Prevention of New Disease X and Investigation of the Origin of COVID-19
- Why Botulinum Toxin Reigns as One of the Deadliest Poisons?
- FDA Approves Pfizer’s One-Time Gene Therapy for Hemophilia B: $3.5 Million per Dose
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
Why does MRI often underestimate the size of prostate tumors?
- Red Yeast Rice Scare Grips Japan: Over 114 Hospitalized and 5 Deaths
- Long COVID Brain Fog: Blood-Brain Barrier Damage and Persistent Inflammation
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- What is the difference between Atorvastatin and Rosuvastatin?
- How long can the patient live after heart stent surgery?
Why does MRI often underestimate the size of prostate tumors?
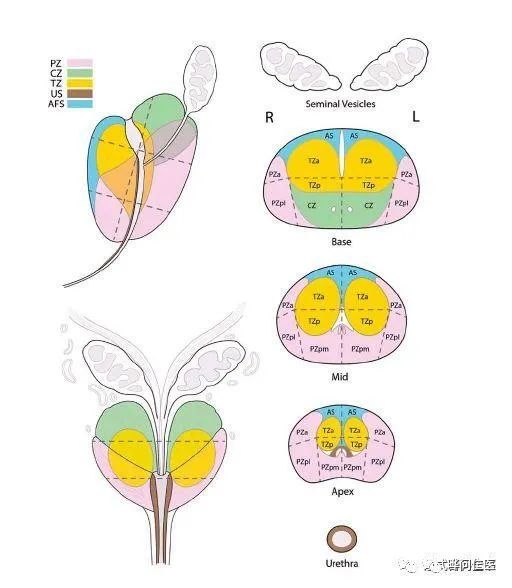
The prostate is the largest substantial organ in the accessory glands of the male genitalia.
They are unpaired substantial glands that surround the root of the urethra and resemble a slightly flat chestnut in shape and size.
The upper end is wide and the lower end is thin, close to the rectum, and can be palpable through the rectal examination.
The prostate is the largest substantial organ in the accessory glands of the male genitalia. They are unpaired substantial glands that surround the root of the urethra and resemble a slightly flat chestnut in shape and size.
The upper end is wide and the lower end is thin, close to the rectum, and can be palpable through the rectal examination.
Glandular tissue in the elderly gradually degenerates, hyperplasia of connective tissue in the gland, forming prostate hyperplasia, compression of the urethra, can cause dysuria.
Early prostate cancer usually has no symptoms, so it is easy to misdiagnose prostate cancer as benign prostatic hyperplasia, which is called prostatic hypertrophy, and it is easy to delay the best treatment time.
Therefore, the diagnosis of prostate cancer is particularly important. But why does MRI often underestimate the size of prostate tumors?
The influence of MRI on the diagnosis of local prostate cancer
Because certain tumors cannot be detected by radiography or pathology, the use of magnetic resonance imaging (MRI) to detect these invisible tumors is a challenge in the diagnosis of prostate cancer.
The progression and natural course of these lesions are not clear. Scholars from the National Cancer Institute in the United States evaluated MRI occult tumors (MIT) in men with prostate multi-parameter MRI and MRI/transrectal ultrasound (TRUS) fusion-guided biopsy.
A study led by researchers at the Johnson Comprehensive Cancer Center at the University of California, Los Angeles found that magnetic resonance imaging or MRI usually underestimates the size of prostate tumors, which may lead to undertreatment.
The study authors found that when the size of the tumor measured by MRI was small and the PI-RADS score used to classify the lesion in the prostate MRI analysis was low, the possibility of underestimation increased.
Does size matter?
In order for prostate tumor treatment to be successful, both MRI size measurement and PI-RADS score must be accurate because they enable doctors to accurately determine where the tumor ends and where the surrounding normal healthy tissue begins. The size of the lesion can be used as an indicator of the number of clinical puncture points for prostate cancer.
MRI/US fusion guided prostate biopsy (FBx) has more applications and fewer puncture points than standard prostate biopsy, and can detect clinically significant prostate cancer.
The size of the image plays an important role in determining the degree of suspiciousness (PI-RADS) of the lesion identified by MRI.
However, the size of the tumor may present challenges for accurately characterizing the lesion.
A study by the National Cancer Institute tried to determine whether there is a size boundary that can accurately characterize the lesion as a clinically significant cancer through a single biopsy puncture point.
The data shows that for lesions smaller than 0.65 cm and larger than 1.70 cm, clinically significant prostate cancer can be confirmed by a single targeted biopsy, while only 33.5% of the lesions (21% of patients) require dual-point targeted biopsy.
Negative fusion and post-biopsy detection
Clinically significant prostate cancer
MRI is commonly used to diagnose and manage prostate cancer. It is also increasingly used as a means to map and guide new, highly intensive therapies that use freezing (cryotherapy), ultrasound (HIFU) and heating (laser ablation) to destroy cancerous tissue in the prostate. At the same time preserve healthy tissue.
The researchers compared 441 men who were treated for prostate cancer and compared the tumor size measured by MRI with the actual tumor size after prostate resection.
Improving the ability to better predict the ablation margin will make the treatment of male prostate cancer more successful and help reduce the incidence of prostate cancer treatment.
MRI/ultrasound fusion biopsy of the prostate enhances the clinically important prostate cancer (csPCa) detection. However, the findings of negative fusion and negative systematic biopsy in patients with imaging suspicious lesions raise the issue of false positive imaging or false negative biopsy.
The researchers reviewed the data of 400 patients underwent MRI/transrectal ultrasound-guided fusion biopsy. All images were graded according to the Prostate Imaging Report and Data System Version (PIRADS) 2.0.
The study found that despite the negative initial fusion/systemic biopsy, at least 10% of patients were subsequently diagnosed with clinically significant PCa. After a negative fusion biopsy, for patients with low PSAd, repeated MRI can reveal a higher rate of PIRADS lesion disappearance.
Why does MRI often underestimate the size of prostate tumors?
(source:internet, reference only)
Disclaimer of medicaltrend.org



