Is there any change on tumor radioimmunotherapy in past 10 years?
- Normal Liver Cells Found to Promote Cancer Metastasis to the Liver
- Nearly 80% Complete Remission: Breakthrough in ADC Anti-Tumor Treatment
- Vaccination Against Common Diseases May Prevent Dementia!
- New Alzheimer’s Disease (AD) Diagnosis and Staging Criteria
- Breakthrough in Alzheimer’s Disease: New Nasal Spray Halts Cognitive Decline by Targeting Toxic Protein
- Can the Tap Water at the Paris Olympics be Drunk Directly?
Is there any change on tumor radioimmunotherapy in past 10 years?
- Should China be held legally responsible for the US’s $18 trillion COVID losses?
- CT Radiation Exposure Linked to Blood Cancer in Children and Adolescents
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- How long can the patient live after heart stent surgery?
Is there any change on tumor radioimmunotherapy in past 10 years?
Preface
In the past ten years, the application of monoclonal antibodies carrying radionuclides in cancer treatment ( diagnosis and therapy ) has been in clinical research, and more and more radioactivity with different properties ( half-life, emission spectrum, particles or electrons ) The nuclides are evaluated.
However, so far, the selection of RIT radionuclides in clinical trials is limited to I-131, Y-90, Lu-177 and Re-188, Bi-213 and At-211.
In addition, the FDA has only approved two radioimmunotherapy ( RIT ) for targeted therapy of hematological tumors expressing CD20 antigen.
RIT still faces many challenges. Accurate dosimetry is very important for RIT.
In addition to the inherent properties of radionuclides, the properties of antibodies also have an important influence on the different therapeutic effects induced by RIT.
Radiolabeled antibodies that have undergone internalization are better than targeted Non-internalizing antibodies to the cell membrane cause more DNA double-strand breaks.
In addition, the RIT application of solid cancer faces major problems, such as radiotoxicity due to the permeability of antibodies and the need for a large therapeutic dose. The new discoveries of antibody engineering and radionuclides are trying to overcome these problems, and RIT is gradually showing A good application prospect.
Overview of RIT Research
Summarizing the 92 RIT research publications published in the past 10 years, it can be found that 67% are related to RIT of non-solid tumors ( 62 studies ), and only 33% are related to RIT research of solid tumors ( 30 studies ), 2013 -The peak was reached in 2014.

The RIT classification of non-solid cancers shows that the research on lymphomas ( including follicular lymphoma, mantle cell lymphoma, Burkitt lymphoma, diffuse large B-cell lymphoma, marginal zone lymphoma and Hodgkin’s lymphoma ) is very Outstanding, accounting for 92.5% of the survey.
In contrast, RIT for solid tumors was evaluated on a wider variety of targets and tumors, with metastatic cancer accounting for 61.9% of all studies.
RIT treatment of hematoma
In the first decade of this century, positive clinical results led the FDA to approve two radioimmune complexes, namely 90 Y- ibritumomab tiuxetan ( Zevalin®, Bayer ) approved in 2002 and 131 I- tositumomab ( Bexxar®, GSK ), both drugs are based on mouse anti-CD20 monoclonal antibodies.
Both are initially suitable for the treatment of patients with relapsed or refractory ( R/R ), low-grade or follicular B-cell non-Hodgkin’s lymphoma ( B-NHL ), including rituximab refractory filtration Patients with vesicular NHL.
After these two drugs were approved, a large number of RIT clinical studies were subsequently conducted.

Follicular lymphoma (FL)
In the first-line treatment of advanced FL, the efficacy and well tolerability of 90 Y -ibritumomab tiuxetan and 131 I -rituximab have been proven .
In FL, the second-stage evaluation of the first-line consolidation program using 90 Y- ibritumomabtiuxetan showed promising results.
Compared with the non-consolidation strategy, the progression-free survival ( PFS ) has a clear advantage. However, the phase III first-line consolidation study using 131 I -tositumomab failed to prove clinical benefit.
Regarding R/R FL, the safety and effectiveness of 90 Y- ibritumomab tiuxetan have been proven in a phase I study. The phase III trial used 131 I- tositumomab to evaluate RIT. However, the trial was terminated early because only 14 patients were included, so important conclusions could not be drawn.
In patients with marginal zone lymphoma ( MZL ), three phase II studies have shown that 90 Y- ibritumomab tiuxetan is also beneficial in first-line or consolidation therapy.
Aggressive B-NHL
In aggressive B-NHL, including transformed low-grade B-NHL, DLBCL, and MCL, studies evaluating anti-CD20RIT have shown that it is well tolerated. In most studies, regardless of the type of aggressive B-NHL, the significant benefits of survival have been emphasized.
However, in a study in MCL, it did not show a significant improvement in survival compared to a regimen involving rituximab.
Despite these promising results, in a phase III clinical trial for patients with chemotherapy-sensitive relapsed DLBCL, 131 I -tositumomab compared with BEAM or rituximab, and showed no difference in PFS and OS.
Other blood diseases
Among non-B-NHL hematomas, stage I anti-CD20 RIT showed good efficacy and tolerability, including MM ( ORR: 73%; CR: 23% ) and R/R Hodgkin’s lymphoma ( 2 cases) CR/12 patients ).
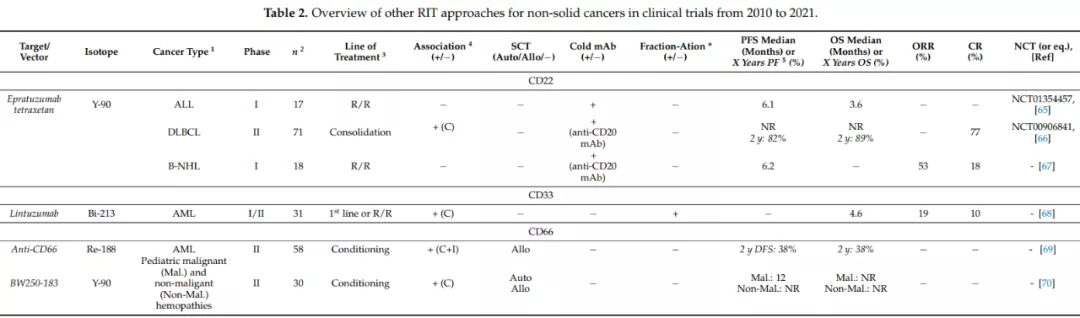
In addition, other strategies besides CD20 have also been explored, for example, the use of Bi-213 anti-CD33 monoclonal antibody in B-NHL, and the use of Re-188 or Y-90 anti-CD66 monoclonal antibody in AML.
RIT treatment of solid tumors
Despite improvements in radionuclide and RIT procedures, RIT treatment of solid tumors is still quite limited. In the past decade, clinical trials using radionuclide-labeled monoclonal antibodies for the treatment of solid tumors have been reduced by a factor of two.
In all published RIT clinical trials, there is a lack of phase III trials, about 50% are phase I trials, and about 40% are phase I/II trials. Most of them only assessed the feasibility and toxicity of RIT, so it is difficult to clearly determine the therapeutic effect of RIT.
Most clinical trial reports on RIT for solid tumors involve a limited number of patients who are already in the metastatic stage and who are resistant to first-line or second-line therapies.
The RIT of hematological tumors mainly focuses on four different antigen targets ( ie CD20, CD22, CD33 and CD66 ). So far, the RIT of solid tumors has tested 12 different antigens, and each antigen is only evaluated once in clinical trials. Two times, thus making it difficult to compare different studies to determine whether RIT is effective.
One reason why RIT is difficult to successfully treat solid tumors is that it relies on the penetration of intact monoclonal antibodies and lower doses.
However, the vascular leakage of tumor vasculature and the presence of highly complex extracellular matrix prevent tumor cells from contacting monoclonal antibodies.
In addition, the hypoxia present in most solid tumors reduces radiation efficiency. Therefore, people began to try some different alternatives.
Alternatives and prospects of traditional RIT
The long half-life of IgG is a major disadvantage of RIT therapy for solid tumors, because the slow penetration of monoclonal antibodies leads to blood toxicity and drug resistance. Currently, two main strategies have been explored to circumvent these problems, both of which are based on improving the pharmacokinetics of carriers carrying radionuclides.
Fragment-based RIT

Fab′
Fab’ was clinically approved by the FDA as early as 1994 to prevent thrombosis during angioplasty ( ReoPro® ).
So far, the FDA, EMA and China have also approved several Fab’ fragment drugs, including cancer treatments such as Ranibizumab. However, so far, no RIT has been approved.
In 2002, in a very small pilot study cohort, patients with colorectal cancer were evaluated with I-131 labeled CEA targeting bivalent Fab’ fragment RIT.
Imaging shows that there are specific signals in patients with tumors expressing CEA.
However, it failed to show significant tumor uptake compared to other organs. In addition, aggregation was observed in three patients, which correlated with the amount of CEA antigen measured in the patient’s serum.
It is worth noting that Fab’ fragments also show some diagnostic potential. For example, the 99m Tc-nofetumimab-merpentan Fab’ fragment ( Verluma® ), which targets pancreatic cancer antigens expressed by cancer cells , was approved by the FDA for the diagnosis of small cell lung cancer in 1992, but was discontinued in 2013.
F(ab′) 2
In 2011, Anascorp® became the first F(ab′) 2 approved by the FDA for the treatment of clinical symptoms of scorpion poisoning. Subsequently, the FDA approved Anavip® in 2015 for the treatment of the coagulation effect of cantharidin poisoning in North America.
Regarding RIT, F(ab’) 2 is the most common type of fragment evaluated in clinical trials. But since 2010, only two are still being studied, CD147 for metastatic solid tumors and tenascin C for Hodgkin’s lymphoma.
In addition to CD147, the targeted therapy of tenascin C and CEA is still in the early clinical evaluation stage (Phase I/II ), involving only a small number of patients. In most cases, the conventional I-131 radiolabel is used.
Several clinical trials have used 131 I -metuximab HAb18G/CD147 F(ab′) 2 ( Licartin® ) as postoperative treatment, or combined with radiofrequency ablation to treat patients with recurrent metastatic hepatocellular carcinoma (HCC).
RIT containing metuximab is associated with mild to moderate hematology/hepatotoxicity, all ≤3 grade; in addition, thyroid function is not impaired, and there is no obvious human anti-mouse antibody ( HAMA ) positive after two cycles of treatment .
In the most recent study, the median OS was between 20 and 60 months, and the 5-year PFS in the treatment group was approximately 43.4%, compared to 21.7% in the control group.
ScFv
In oncology, single-chain antibody fragments have been widely used in chimeric antigen receptor ( CAR ) T cell immunotherapy.
In the RIT clinical trial, the only study describing the use of radiolabeled single-chain antibodies was a phase I trial in 2011, which used a 131 I- CIGB-M3 trivalent single-chain antibody that targeted CEA.
In the evaluation of 17 patients, it had low non-targeted toxicity and low HAMA response. Despite showing good pharmacokinetic results and dosimetry, clinical development has not been carried out so far.

Pre-targeted radioimmunotherapy (PRIT)
Another potential strategy to increase clearance and reduce off-target toxicity is to delay the radionuclide administration of monoclonal antibodies in it through the so-called pre-targeting method, delaying administration from several hours to several days.

This method first administers the complete antibody or fragment conjugate to fully bind to the target, usually several hours to several days before administering the radioactive component to allow time to accumulate in the tumor.
The radioligand and the monoclonal antibody conjugate have Highly specific payload association. In order to obtain a fast reaction, a high affinity between the two ligands is required.
Due to the small size of the radioligand, rapid biodistribution in the blood, and short half-life, PRIT has low non-targeted toxicity to healthy tissues.
In the past 30 years, different PRIT strategies have been developed. The oldest strategy involves high affinity between biotin and streptavidin. Although good results have been achieved in preclinical trials, clinical I/II phase trials have demonstrated the immunogenicity of streptavidin and its non-target binding activity with endogenous biotin.
Another PRIT strategy based on bispecific or multispecific antibodies or fragments was quickly developed. In 2012, a phase II study was conducted on a chimera bispecific human/mouse ( hMN-14×m734 ) F(ab′) 2 which is an anti-CEA×antibody labeled with I-131 DTPA is used to treat patients with medullary thyroid cancer. The administration between bsAbs and 131 I -DTPA was delayed by 4 to 6 days.
The results showed that most patients tolerated PRIT well. In addition, the efficacy of PRIT was proven to control the disease in 76% of patients, with median PFS It was 13.6 months, and the median OS was 43.9 months.
Recently, chimeric (hMN-14×m734) F(ab′) 2 has also shown interesting and promising results in the treatment of metastatic colorectal cancer.
Summary
Although the FDA has approved two RIT drugs, the indications for anti-CD20 RIT have not been expanded in the past ten years, and the number of clinical RIT trials has decreased year by year.
People’s interest in this treatment strategy for hematological malignancies is declining. In addition, in solid tumors, there is currently no RIT verified by the FDA or EMA.
However, it is worth noting that the number of RIT in solid tumors has increased significantly, reaching a peak recently, accounting for more than 50% of ongoing RIT clinical trials.
The combination of a large number of newly discovered targets/antibodies with effective radionuclides indicates that RIT has new application prospects in solid tumors, especially metastatic malignant tumors.
In addition, recent advances in antibody fragment bioconjugation and targeted strategies have given us hope to improve the efficacy of RIT and expand the application of solid tumors in the next ten years.
references:
1.Radioimmunotherapy in Oncology: Overview of the Last Decade Clinical Trials. Cancers (Basel). 2021 Nov; 13(21): 5570.
Is there any change on tumor radioimmunotherapy in past 10 years?
(source:internet, reference only)
Disclaimer of medicaltrend.org
Important Note: The information provided is for informational purposes only and should not be considered as medical advice.



