Spinal tuberculosis: Pay attention to distinguish it from spondylitis!
- A Single US$2.15-Million Injection to Block 90% of Cancer Cell Formation
- WIV: Prevention of New Disease X and Investigation of the Origin of COVID-19
- Why Botulinum Toxin Reigns as One of the Deadliest Poisons?
- FDA Approves Pfizer’s One-Time Gene Therapy for Hemophilia B: $3.5 Million per Dose
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
Spinal tuberculosis: Pay attention to distinguish it from spondylitis!
Spinal tuberculosis: Pay attention to distinguish it from spondylitis! Imaging diagnosis of spinal tuberculosis: pay attention to distinguish it from spondylitis!
Central bone destruction is concentrated in the center of the vertebral body, which is clearer on the lateral radiograph.
Spinal tuberculosis, also known as Pott’s disease, is a secondary disease, about 90% of which are secondary to tuberculosis. The vast majority of the disease is spread through blood. It is more common in children and adolescents, of which over 80% are under 30. The most common site is the spine, which accounts for about 50%, followed by knees, hips, and elbows.
The following is the author’s review of literature, collecting typical cases of spinal tuberculosis encountered in clinical practice, and uncovering the veil of spinal tuberculosis through the angle of imaging.
Case one
A 32-year-old female, fever, stiff neck, difficulty swallowing for 2 weeks, and a history of night sweats for only two years, the results of cervical MR examination are as follows.
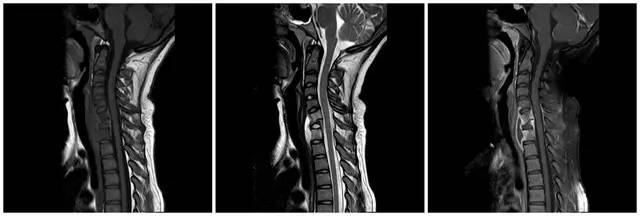
Figure 1 Cervical MRI, followed by sagittal T1WI, T2WI and T1WI after enhancement. The figure shows that the C7 vertebral body becomes flattened, the C6/7 intervertebral disc involvement disappears, and the anterior vertebral body abscess forms. Extensive T2WI edema signals can be seen in C6 and T1 vertebrae
Case two
A 29-year-old man was admitted to the hospital with a history of Horner syndrome, and his neck was found to be enlarged on physical examination. The results of relevant imaging examinations are as follows.
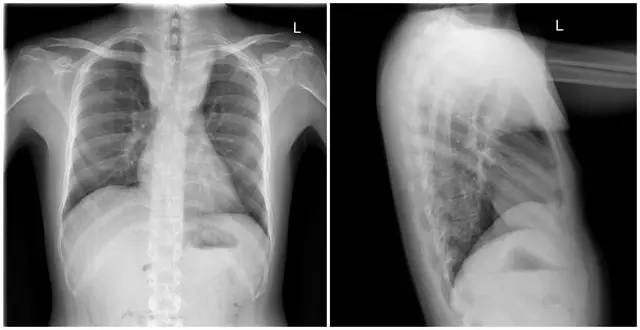
Figure 2 X-ray examination of the front and side view showed that the upper mediastinum was widened, a soft tissue mass was seen in the front of the vertebral body, and the trachea was compressed and shifted forward
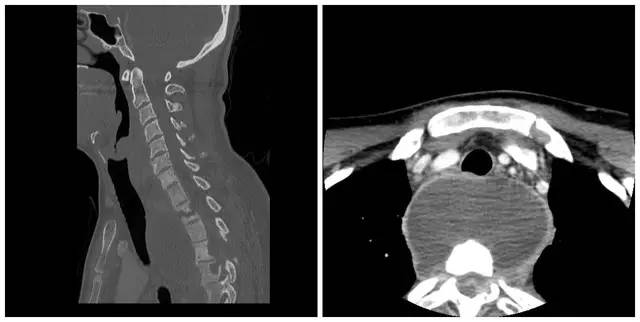
Figure 3 CT examination results show that the upper thoracic spine has multiple vertebral body worm-like damages, and the formation of a large low-density edge in front of the vertebral body enhances cold abscess

Figure 4 MR examination results are consistent with CT. The image above is the image after sagittal T1WI enhancement, showing that the lesion is wider than CT: the corresponding vertebral body and appendages, and surrounding soft tissues are all affected
Case three
Male, 50 years old, with unknown clinical symptoms. The results of imaging examination are as follows.
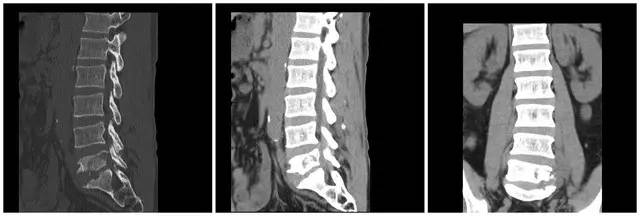
Figure 5 CT results of the lumbar spine showed that the bones of the L5 and S1 vertebrae were destroyed

Figure 6 MRI examination results show that L5 and S1 vertebrae can see abnormal signals of long T1 long T2 in slices, and the enhancement shows obvious heterogeneous enhancement, mainly in the L5 vertebra. The degree of intervertebral disc involvement is relatively light
Case Four
A 30-year-old male with a history of leg weakness. The imaging results are as follows.

Figure 7 Lumbar anterior and lateral radiographs show that the T12 and L1 vertebrae are abnormal

Figure 8 Lumbar MRI results showed that T12 bone collapsed, the lumbar spine was kyphotic, T11-12, L1-2 vertebral bodies and appendages showed abnormal signals of long T1 long T2, and T12/L1 intervertebral discs were obviously involved. The above lesions showed obvious heterogeneous enhancement, the spinal cord was compressed and thinned, and abscess formation was seen in the soft tissues of the back at the corresponding level
Imaging signs of spine tuberculosis
1. X-ray
It is manifested as vertebral bone destruction, narrowing of the intervertebral space, angular deformity and cold abscess formation. It is more common in the lower thoracic spine and upper lumbar spine, often involving 2 to 3 connected vertebral bodies. The lesions are mainly osteolytic destruction , Bone hyperplasia and sclerosis is not significant.
2. CT plain scan
It shows that the cancellous bone of the vertebral body is destroyed, the bone cortex loses its integrity, and there are dead bones and slight bone hyperplasia and collapse. The intervertebral disc is relatively intact in the early stage, and the intervertebral disc is destroyed later, the gap is narrowed, and the abscess is single or multi-chambered.
3. MRI examination
It has the value of early diagnosis. It can show abnormal signals at the stage of inflammatory infiltration and can also be used to observe whether the spinal cord is compressed and degenerated.
【Diagnosis Essentials】
1. The cancellous bone destruction of the vertebral body, the interruption of the bone cortex, the formation of dead bone, slight bone hyperplasia and the collapse of the vertebral body. The intervertebral disc is relatively intact in the early stage, and then it is destroyed and the intervertebral space becomes narrow.
2. The marginal type first invades the intervertebral disc and the endplate, and the accessory type mainly destroys the accessory bone.
3. Abscesses are mostly unilocular or multilocular low-density, the center is not enhanced, and the abscess wall is irregularly ring-shaped.
Differential diagnosis
1. Brucella spondylitis
2. Suppurative spondylitis
Discuss
Vertebral tuberculosis can be divided into central type and edge type according to the location of the vertebral body: the central type is more common in children, and the lesion starts in the cancellous bone of the vertebral body. There are often dead bones and cavities. Due to the progress of small vertebral diseases It is very easy to invade the entire vertebral body and intervertebral disc; the marginal type starts from the left and right sides and the front and back of the upper and lower edges of the vertebral body. Pathological compression fractures can occur when the diseased vertebra is compressed. The anterior compression is mostly wedge-shaped, bone marrow slices or sequestered bones Can be squeezed into the spinal canal to compress the spinal cord or nerve roots.
Central bone destruction is concentrated in the center of the vertebral body, which is clearer on the lateral radiograph. Soon the vertebral body was compressed into a wedge shape, narrow in the front and wide in the back. It can also invade the intervertebral disc and involve adjacent vertebral bodies. Marginal bone destruction is concentrated on the upper or lower edge of the vertebral body, and quickly invades the intervertebral disc, manifested by the destruction of the vertebral body endplate and progressive intervertebral stenosis, and involves two adjacent vertebral bodies. The bone destruction and wedge compression of the edge type are not as obvious as the center type, so the kyphosis is not heavy.
(source:internet, reference only)
Disclaimer of medicaltrend.org



