Harvard: The response rate of ketamine in the treatment of refractory major depression was 55.4%
- Why Lecanemab’s Adoption Faces an Uphill Battle in US?
- Yogurt and High LDL Cholesterol: Can You Still Enjoy It?
- WHO Releases Global Influenza Vaccine Market Study in 2024
- HIV Infections Linked to Unlicensed Spa’s Vampire Facial Treatments
- A Single US$2.15-Million Injection to Block 90% of Cancer Cell Formation
- WIV: Prevention of New Disease X and Investigation of the Origin of COVID-19
Harvard: The response rate of ketamine in the treatment of refractory major depression was 55.4%
- Red Yeast Rice Scare Grips Japan: Over 114 Hospitalized and 5 Deaths
- Long COVID Brain Fog: Blood-Brain Barrier Damage and Persistent Inflammation
- FDA has mandated a top-level black box warning for all marketed CAR-T therapies
- Can people with high blood pressure eat peanuts?
- What is the difference between dopamine and dobutamine?
- How long can the patient live after heart stent surgery?
NEJM: Breakthrough! The Harvard team found that the response rate of ketamine in the treatment of refractory major depression was 55.4%, which was not inferior to electroconvulsive therapy.
For treatment-resistant major depressive disorder (generally defined as poor response to two or more antidepressant medications), electroconvulsive therapy (ECT) is one of the most effective and rapid ECT has not been fully promoted and used because of concerns about adverse events of cognitive impairment and cognitive impairment [1-3].
Ketamine, used for sedation, analgesia, and anesthesia, has a rapid antidepressant effect observed in patients with major depressive disorder and treatment-resistant major depressive disorder when administered at sub-anesthetic doses [4,5]. Ketamine neither requires general anesthesia nor is associated with clinically significant memory impairment [6] and thus has potential as an alternative to ECT, however, ketamine causes temporary changes in sensation and thinking and should only be used in nonpsychotic refractory patients with major depressive disorder.
In order to verify the effectiveness and safety of ketamine compared with ECT, a research team from Harvard Medical School and other medical research institutions conducted a prospective, randomized, open-label, non-inferiority trial.
The results of the trial showed that the response rate of ketamine in the treatment of patients with non-psychiatric refractory major depression was 55.4%, which was non-inferior to ECT (41.2%), with a higher remission rate and less impact on cognitive ability and life. Quality improved.In terms of adverse events, ECT was associated with musculoskeletal adverse events and ketamine was associated with dissociative symptoms. The findings were published in The New England Journal of Medicine [7].
Participants were randomized 1:1 at 5 urban community hospitals/VA hospitals/university medical centers in the US to receive either ketamine or ECT during a 3-week initial treatment phase to determine response to treatment (Defined as a decrease in the Quick Self-Rating Scale of Depression Symptoms [QIDS-SR-16] score of at least 50%), participants who responded to treatment entered a 6-month follow-up phase.
Modified intention-to-treat (mITT) participants totaled 365, 195 in the ketamine group and 170 in the ECT group. The average age of the participants was 46 years, 51.1% were female, 88.1% were white, the severity of the current depressive episode was moderate to severe, the median duration was 2.0 years, 77.9% had a family history of depression, 39.0% had Suicide attempt.
For the primary outcome, 55.4% (108/195) of participants in the ketamine group responded to treatment based on change in QIDS-SR-16 score, compared with 41.2% (70/170) in the ECT group, a difference of 14.2% compared to ketamine ECT was non-inferior (p<0.001).
With regard to the secondary outcome, 50.8% of participants in the ketamine group responded to treatment, as measured by change in Montgomery Depression Rating Scale (MADRS) score, compared with 41.1% in the ECT group, a difference of 9.3%. Both QIDS-SR-16 and MADRS scores decreased gradually after the treatment started. According to the change of QIDS-SR-16 score (score ≤ 5 points), 32.3% of the ketamine group achieved remission, and 20% of the ECT group achieved remission. According to the change of MADRS score (score ≤ 10 points), the proportions of remission were 37.9% and 21.8%, respectively .
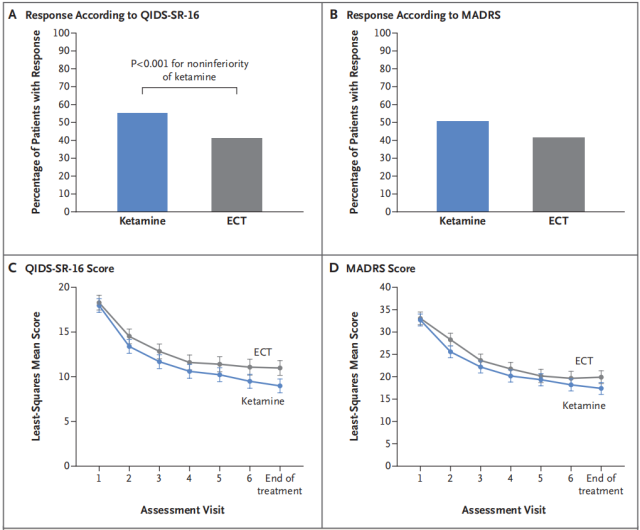
Ketamine and ECT treatment response rates as assessed by changes in QIDS-SR-16 and MADRS scores (A and B)
Changes in QID S-SR-16 and MADRS scores over time during treatment (C and D)
At the end of treatment, memory function was worse in the ECT group than in the ketamine group according to the Global Memory Self-Evaluation (GSE-My) score (mean score 3.2±0.1 vs. 4.2±0.1) and remained worse at the end of the 6-month follow-up period.
According to the subjective memory impairment scale (SMCQ) score, the cognitive symptoms in the ketamine group were less than those in the ECT group (mean score difference was 9.0), and gradually recovered during the follow-up period.
According to the revised Hopkins University Verbal Learning Test (HVLT-R), scores on the delayed recall (20-minute delay after memorizing a word in the test) component of the ECT group decreased more than the ketamine group (-9.7±1.2 vs. -0.9±1.1), but gradually recovered during the follow-up period.
According to the 16 quality of life scores, both groups increased from baseline to the end of treatment, and the increases were similar (12.3 vs. 12.9), and remained stable during the follow-up period.
At least one moderate or severe adverse event (AE) occurred in 25.1% of the participants in the ketamine group and 32.4% in the ECT group, and there were no deaths.
The incidence of musculoskeletal AE was significantly higher in the ECT group than in the ketamine group (5.3% vs. 0.5%), and the dissociative symptom score was higher in the ketamine group than in the ECT group.
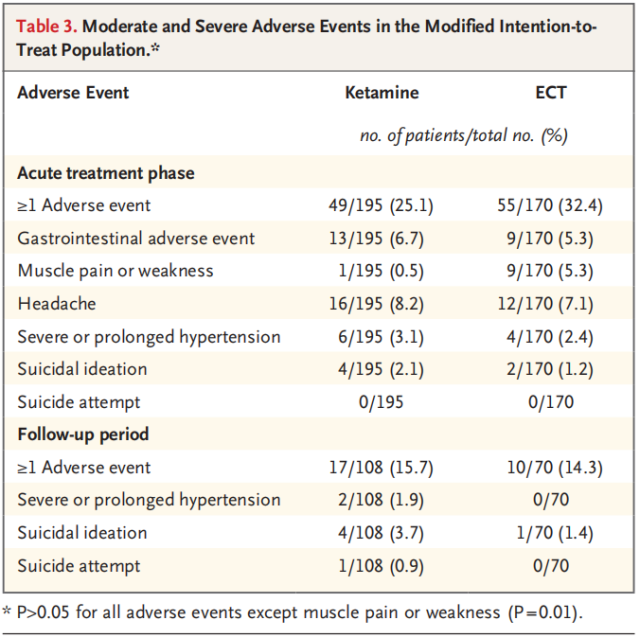
Summary of Adverse Events in the Ketamine and ECT Groups
During follow-up, 19.0% and 35.4% of participants in the ketamine and ECT groups relapsed (QIDS-SR-16 score >11) at month 1, increasing to 34.5% and 56.3% at month 6.
Overall, this study demonstrates the non-inferiority of ketamine to ECT in the treatment of patients with treatment-resistant major depressive disorder.
The researchers note that the response and remission rates of ECT in this trial were lower than in other studies, which may be due to the fact that, in previous studies, the effectiveness of ECT was more in older, major depressive patients with psychiatric illness, hospitalized Future studies are needed to determine whether ketamine is equally non-inferior to the elderly, bipolar disorder, and emergency department inpatients.
references:
[1] Espinoza RT, Kellner C H. Electroconvulsive therapy[J]. New England Journal of Medicine, 2022, 386(7): 667-672.
[2] Lisanby S H. Electroconvulsive therapy for depression[J]. New England Journal of Medicine, 2007, 357(19): 1939-1945.
[3] Ross EL, Zivin K, Maixner D F. Cost-effectiveness of electroconvulsive therapy vs pharmacotherapy/psychotherapy for treatment-resistant depression in the United States[J]. JAMA psychiatry, 2018, 75(7): 713-722.
[4] Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients[J]. Biological psychiatry, 2000, 47(4): 351-354.
[5] Zarate CA, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression[J]. Archives of general psychiatry, 2006, 63(8): 856-864.
[6] Rasmussen KG, Lineberry TW, Galardy CW, et al. Serial infusions of low-dose ketamine for major depression[J]. Journal of Psychopharmacology, 2013, 27(5): 444-450.
[7] Anand A, Mathew SJ, Sanacora G, et al. Ketamine versus ECT for Nonpsychotic Treatment-Resistant Major Depression[J]. New England Journal of Medicine, 2023.
Harvard: The response rate of ketamine in the treatment of refractory major depression was 55.4%
(source:internet, reference only)
Disclaimer of medicaltrend.org
Important Note: The information provided is for informational purposes only and should not be considered as medical advice.



