Antigen selection for diagnosis of Epstein-Barr (EB) virus
- Aspirin: Study Finds Greater Benefits for These Colorectal Cancer Patients
- Cancer Can Occur Without Genetic Mutations?
- Statins Lower Blood Lipids: How Long is a Course?
- Warning: Smartwatch Blood Sugar Measurement Deemed Dangerous
- Mifepristone: A Safe and Effective Abortion Option Amidst Controversy
- Asbestos Detected in Buildings Damaged in Ukraine: Analyzed by Japanese Company
Antigen selection for diagnosis of Epstein-Barr (EB) virus
Antigen selection for diagnosis of Epstein-Barr (EB) virus. The laboratory diagnosis of Epstein-Barr virus relies on the specific antibody profile. The correct choice of protein types is a necessary condition for the development of test kits.
Editor’s note:
Epstein-Barr virus infection is widely distributed around the world. After it infects the body, it lurks in the host cell and is reactivated when the host’s immune system is damaged.
COVID-19 has ravaged the world for more than a year. With the in-depth study of SARS-CoV-2, scientists have discovered that infection with SARS-CoV-2 can cause a decline in human immunity. In addition, it has been reported that the activation of Epstein-Barr virus will affect the treatment of CoVID-19, and the synergistic effect of Epstein-Barr virus and SARS-CoV-2 will increase the mortality rate.
We believe that with the continuous efforts of scientific researchers, these problems can be solved one by one. At present, under the background that infection with SARS-CoV-2 will lead to a decline in human immunity, more attention should be paid to the prevention and treatment of latent infections such as Epstein-Barr virus.
Epidemiology and laboratory diagnosis of Epstein-Barr virus
EB virus infection is very common. Official WHO data shows that about 95% of adults worldwide are infected with Epstein-Barr virus. Not only adults, but minors, especially children, are more affected by the Epstein-Barr virus. Because the immune system is not yet mature, minors are more likely to cause serious diseases after being infected with the Epstein-Barr virus. Studies have found that primary Epstein-Barr virus infection in developing countries usually occurs in an asymptomatic or clinically non-specific manner during childhood. The EB virus seroprevalence rate of Chinese children exceeds 50% before the age of 3, and exceeds 90% after the age of 8.
The EB virus establishes a lifelong latent infection after the primary infection, which can be activated and proliferate in a large amount under certain circumstances. The impaired immune system of the body mentioned above is one of the important activating factors. EB virus primary infection or recurrent infection can cause different diseases. The EB virus diagnosis and treatment guidelines or expert consensus affirm the important role of serological testing. Determine the type of disease by detecting the specific antibody profile.
Epstein-Barr virus serological diagnosis—specific antibody profile
It can be seen from the foregoing that the serological diagnosis of Epstein-Barr virus relies on specific antibody profiling, combined with the detection of multiple markers, and comprehensively judges the type of disease and infection status. This is different from the clinical diagnosis of other pathogens-judged by the specific antibodies of a single marker (IgG/IgM/IgA). In the clinical diagnosis of Epstein-Barr virus, the simultaneous detection of several EB virus-specific antibodies in the patient’s serum can improve the sensitivity and specificity of diagnosing primary Epstein-Barr virus infection, and help determine primary Epstein-Barr virus infection, past infection or past EB virus infection is reactivated. (According to “Expert Consensus on Laboratory Diagnosis and Clinical Application of Epstein-Barr Virus Infection (2018)”)
In order to understand the specific antibody spectrum of the Epstein-Barr virus more intuitively, we found the kinetic diagram of the serum antibody of the Epstein-Barr virus. Figure 1. After the body is infected with EB virus, B lymphocytes are activated and transformed into plasma cells, secreting various anti-viral antibodies. The viral capsid protein (VCA) is expressed during the proliferation of the virus and is related to the replication of the virus. The VCA-IgM antibody appears at the beginning of the infection and usually disappears in 2-3 months.
Because the VCA-IgM antibody appears transiently, it is generally considered to be a hallmark antibody of acute EB virus infection. The VCA-IgG antibody also appears with the VCA-IgM antibody at the initial stage of infection, but it can persist in the body for many years or life, so it cannot be used to distinguish acute infections from previous infections. Epstein-Barr virus nucleoprotein (EBNA) is produced during the recovery period of the primary infection, and EBNA-IgG antibody positivity is often regarded as a specific indicator of previous infections.
In addition, the early viral protein (EA) is expressed during the period of virus proliferation and is related to virus replication. EA-IgG antibody appears after VCA-IgM and VCA-IgG antibodies, and lasts for a few weeks after reaching the peak. It can be used as a diagnostic indicator of acute infection (including late primary infection and reactivation of previous infections).
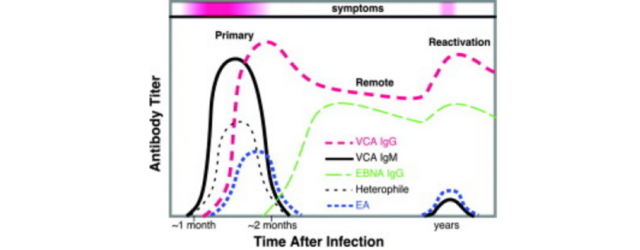
Figure 1: EB virus serum antibody dynamics diagram
Antigen selection of Epstein-Barr virus detection reagents
For the development of Epstein-Barr virus detection reagents, the correct choice of antigen type is a prerequisite.
Epstein-Barr virus can encode a variety of structural proteins, including VCA, EA, and EBNA. The current research on the mechanism of EB virus infection is in-depth. Studies have found that after the body is infected with the Epstein-Barr virus, it mainly produces an immune response against the three proteins of VCA, EA and EBNA. Figure 2 is the protein map of the Epstein-Barr virus. Studies have found that VCA-p18, VCA-p23, EA-p54, EA-p138 and EBNA-p72 are viral proteins that mainly cause immune responses and are suitable for disease diagnosis.
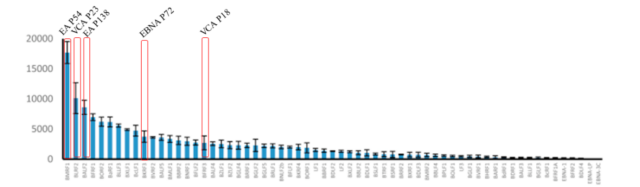
Figure 2: The protein map of the Epstein-Barr virus
In the selection of VCA antigen, there are different protein usage strategies for detecting specific IgG or IgM. VCA-p18 is highly immunogenic in humans and contains B cell epitopes present in the carboxyl region. VCA-p23 can display VCA antibody profile in serological analysis. Studies have found that P18 is used to detect IgM, and P18+P23 is used to detect IgG, and its effect is better. As shown in Figure 3.
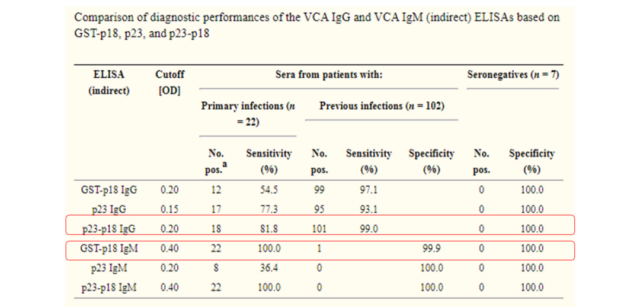
Figure 3: Selection of EB virus VCA protein
In addition, EA-p54 and EA-138 are used in combination, and EBNA-p72 is used alone. The immunoreactivity of these two groups of antigens has also been proved to have high sensitivity. As shown in Figure 4.
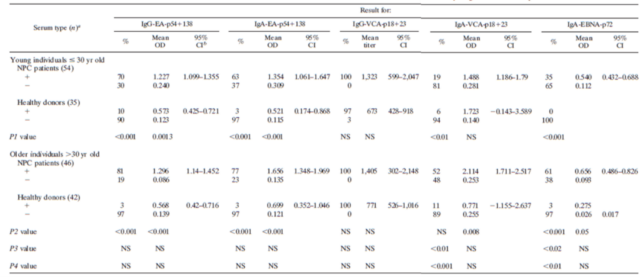
Figure 4: Reactivity of EA-p54+138 and EBNA-p72 protein
Sum up
The laboratory diagnosis of Epstein-Barr virus relies on the specific antibody profile. The correct choice of protein types is a necessary condition for the development of test kits. VCA, EA and EBNA are viral proteins that mainly cause immune responses.
In order to achieve the best results, it is recommended that VCA-p18 is used to detect specific IgM, VCA-p18+p23 is used to detect specific IgG, EA-p54+p138 is used to detect specific IgG, and EBNA-p72 is used to detect specific IgG. Sex antibody.
(source:internet, reference only)
Disclaimer of medicaltrend.org



